Intervention of the Month Intervention of the Month
|
|
|
|
Drug-Eluting Stent May Be Only Tool For Intractable In-Stent Restenosis
Young Joon Hong, MD, PhD, Young Keun Ahn, MD, PhD, FSCAI and
Myung Ho Jeong, MD, PhD, FACC, FESC, FSCAI
The Heart Center of Chonnam National University Hospital, Gwangju, Korea
|
 |
CASE
|
|
A 51-year-old man admitted for the follow-up coronary angiogram (CAG) after Cypher stent implantation for the fifth in-stent restenosis (ISR).
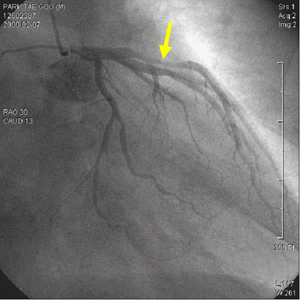
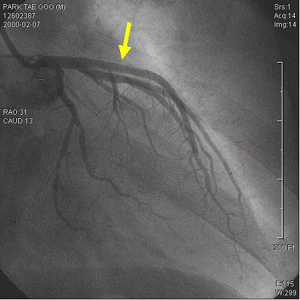
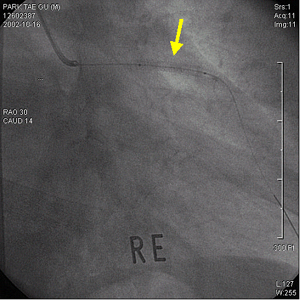
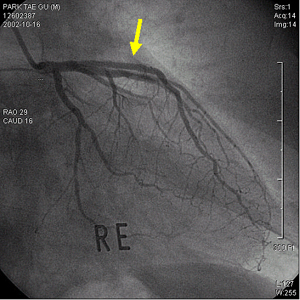
On February 2000, he visited to Chonnam National University Hospital for acute anterior ST-segment elevation myocardial infarction (ASTEMI). His electrocardiogram (ECG) showed ST-segment elevation in V1-5. After thrombolytic therapy using recombinant tissue plasminogen activator, CAG and successful stent implantation for significant stenosis from proximal left anterior descending artery (LAD) to middle LAD using 3.0*27 mm MAC stent was performed (Fig. 1). On January 2001, recurrent chest pain developed. His ECG showed ST-segment elevation in V1-5. CAG revealed type IV (total) ISR in proximal LAD, so, plain old balloon angioplasty (POBA) using 3.0*20mm balloon for first ISR was performed. On December 2002, recurred chest pain was developed. His ECG showed no ST-T changes, but, CAG revealed type II (diffuse) ISR. So, brachytherapy with Rhenium for second ISR was performed for 300 seconds at 6 atm using 3.0*20 mm balloon (Fig. 2). On March 2003, recurred chest pain developed, again. His ECG showed ST-segment elevation in V1-4. CAG revealed type IV ISR, so, brachytherapy failure was occurred. Plain old balloon angioplasty (POBA) using 3.0*20 mm balloon and 3.0*18 mm Core stent implantation distal to previously implanted MAC stent for third ISR was performed (Fig. 3). On July 2003, chest pain recurred again. His ECG showed ST-segment elevation in V3-5. CAG revealed type II ISR, so, plain old balloon angioplasty (POBA) using 3.0*20 mm balloon for forth ISR was performed. On April 2004, recurred chest pain was developed. His ECG showed no ST-T changes. CAG revealed type II ISR in proximal and middle LAD stent. And thus 3.0*33 mm Cypher stent implantation was performed for the fifth ISR (Fig. 4). On July 2004, he received follow-up CAG and CAG showed no ISR (Fig. 5).
Drug-eluting stent may be an only tool for brachytherapy failure and intractable recurrent ISR.
|
| |
|
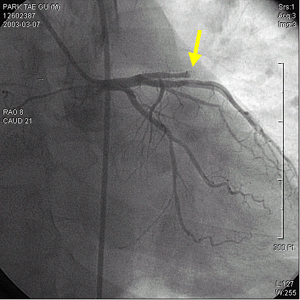
Fig. 1. A diagnostic coronary angiogram (CAG) revealed successful thrombolysis state and critical stenosis from proximal proximal left anterior descending artery (LAD) to middle LAD. After successful stent implantation using 3.0*27 mm long MAC stent, final CAG showed no residual stenosis with good distal flow.
|
| |
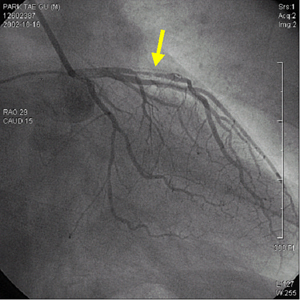
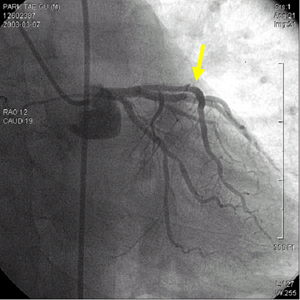
Fig. 2. Second in-stent restenosis (ISR). A coronary angiogram (CAG) revealed type II ISR. Brachytherapy with Rhenium was performed for 300 seconds at 6 atm using 3.0*20 mm balloon. Final CAG showed no residual stenosis with good distal flow.
|
| |
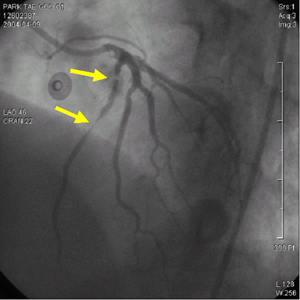
Fig. 3. Third in-stent restenosis (ISR). A coronary angiogram (CAG) revealed type IV ISR, so, brachytherapy failure was occurred. Plain old balloon angioplasty (POBA) using 3.0*20 mm balloon and 3.0*18 mm Core stent implantation distal to previously implanted MAC stent was performed. Final CAG showed no residual stenosis with good distal flow.
|
| |
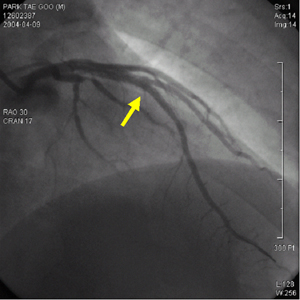
Fig. 4. Fifth in-stent restenosis (ISR). A coronary angiogram (CAG) revealed type II ISR in proximal and middle left anterior descending artery stent. A 3.0*33 mm Cypher stent implantation was performed. Final CAG showed no residual stenosis with good distal flow.
|
| |
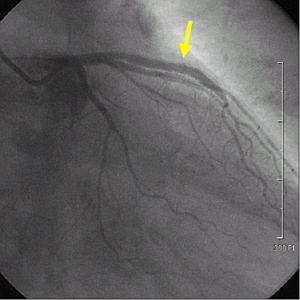 Fig. 5. On follow-up coronary angiogram performed one week later after stenting, the stent of left anterior descending artery was patent and narrowings of the ostium of left circumflex and distal left main artery were not observed.
Fig. 5. On follow-up coronary angiogram performed one week later after stenting, the stent of left anterior descending artery was patent and narrowings of the ostium of left circumflex and distal left main artery were not observed.
|
|
| |
☞ 질문이나 의견이 있으시면 회원들의 공간
 에 글을 써주시기 바랍니다. 에 글을 써주시기 바랍니다. ▲Top
|
|