| нЩНмД±мІД, мШ§мЮђмЫР, к∞ХмДЭлѓЉ, мЬ§мҐЕм∞ђ, мЫРнШЄмЧ∞, мЭімГБнХЩ, л∞ХмД±нХШ, мЮ•мЦСмИШ, м†ХлВ®мЛЭ л∞П KorHF Registry мЧ∞кµђмЮРлУ§ |
Background:
This study hypothesized that bundle branch block (BBB) patterns would be associated with clinical outcomes in hospitalized patients with acute heart failure (AHF).
Methods and Results:
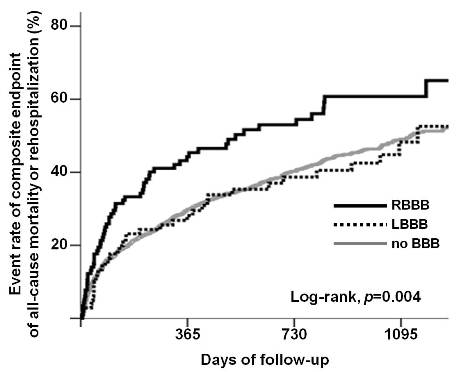
We analyzed 2,202 patients enrolled in the Korean Heart Failure (KorHF) Registry between June 2004 and April 2009 to compare clinical outcomes among right BBB (RBBB, 5.4%), left BBB (LBBB, 4.9%), and no BBB (89.7%) on admission electrocardiogram. The primary composite endpoint was all-cause mortality or rehospitalization. During the median follow-up period of 572 days, the 3-year event rate of the composite endpoint was significantly higher in the patients with RBBB than those with LBBB or no BBB (65.1% vs. 49.9% vs. 49.3%, log-rank, p=0.004). Multivariate analysis demonstrated a significant increased rehospitalization risk for the patients with RBBB vs. LBBB (hazard ratio (HR)=3.07, p=0.001) and the patients with RBBB vs. no BBB (HR=2.22, p<0.001). However, regarding all-cause mortality, there was no significant difference in the patients with RBBB vs. LBBB (HR=2.19, p=0.062) and marginal significance in the patients with RBBB vs. no BBB (HR=1.63, p=0.049). In terms of reduced left ventricular (LV) systolic function (LV ejection fraction вЙ§ 40%), the increased risk of the composite endpoint was pronounced in the patients with RBBB vs. LBBB (HR=2.28, p=0.001).
Conclusions:
RBBB but not LBBB is a significant predictor of all-cause mortality or rehospitalization in hospitalized patients with AHF, especially with reduced LV systolic function.
|