Background: Long-term outcomes of isolated significant tricuspid regurgitation (TR) without significant left-side heart disease remain to be clearly demonstrated.
Methods: We enrolled 547 consecutive patients (age: 64±14 years) with isolated significant TR. Initial clinical and echocardiographic characteristics and clinical outcomes were analyzed for 5.6±2.1 years.
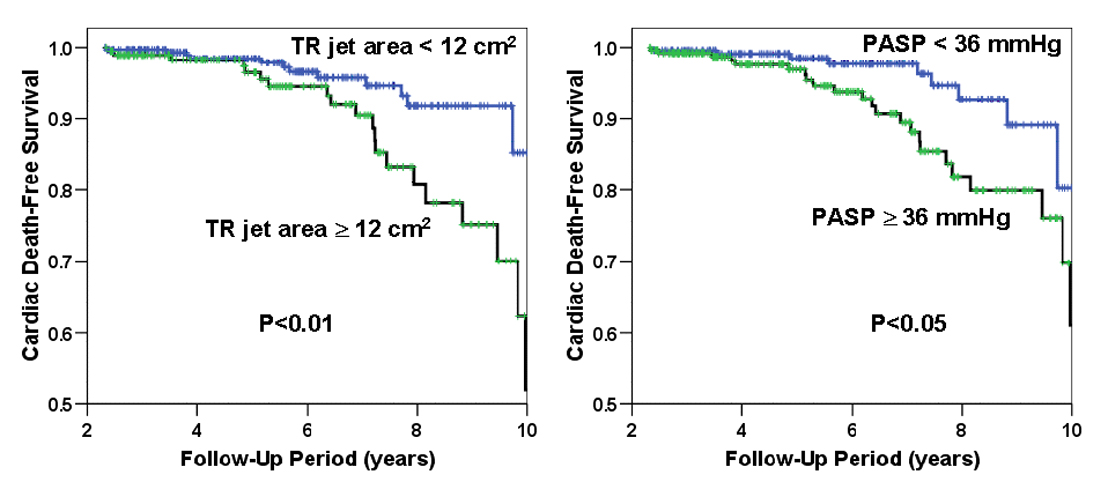
Results: Survival rate was not different between 39 patients who underwent tricuspid valve (TV) surgery and 508 patients who did not (p=0.48). Of 508 patients without TV surgery, 32 patients (6.3%) died with cardiac cause during the follow-up period. Those patients were older (71¬±16 vs. 64¬±13 years, p<0.05) and showed initial larger TR jet area (15¬±7 vs. 12¬±4 cm2, p<0.05), and higher pulmonary artery systolic pressure (PASP, 46¬±22 vs. 39¬±16 mmHg, p<0.05). By adjusting other baseline characteristics using Cox proportional hazard model, age (HR; 1.045, 95% CI: 1.013–1.078), initial TR jet area (HR; 1.110, 95% CI; 1.061–1.160), and PASP (HR; 1.025, 95% CI; 1.009–1.042) were independent predictors of cardiac mortality. Mortality rates did not differ between patients with organic and functional TR. Initial TR jet area вЙ•12 cm2 and PASP вЙ•36 mmHg were best cut-off values for predicting cardiac mortality (Fig).
Conclusions: Severity of TR and pulmonary hypertension are prognostic factors independent of age in medically-managed patients with isolated significant TR. The results may suggest an optimal surgical timing in these patients.
|