BACKGROUND: Although genetic polymorphisms of cytochrome P450 (CYP) and P-glycoprotein may be related with reduced response to clopidogrel, it is not well known whether these polymorphisms can affect the antiplatelet response of intensified antiplatelet therapy. We evaluated the influences of genetic polymorphisms on platelet inhibition with adjunctive cilostazol to dual antiplatelet therapy (triple antiplatelet therapy) and high maintenance-dose (MD) clopidogrel of 150 mg/day.
METHODS: Genotyping for CYP2C19 (*2 or *3), CYP3A5, CYP2B6, and ABCB1 variants was performed in patients on chronic adjunctive cilostazol (triple group; n = 120) and high MD clopidogrel (high-MD group; n = 126) after percutaneous coronary intervention. Residual platelet reactivity (PR) was assessed with conventional aggregometry and VerifyNow assay in chronic phase of antiplatelet therapy (вЙ• 1 mo). High post-clopidogrel platelet reactivity (HPPR) was defined as maximal PR (PRmax) вЙ• 50% with 5 umol/I ADP stimuli.
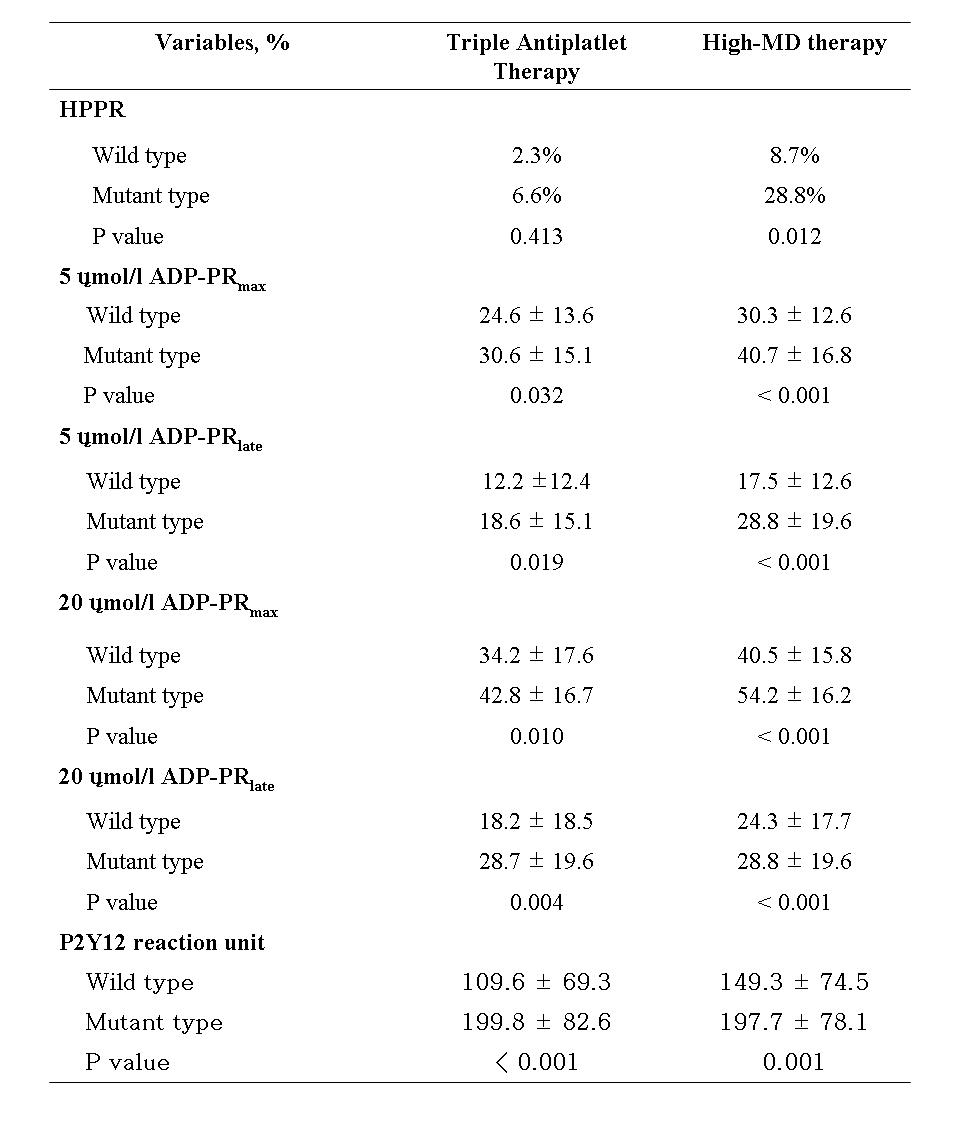
RESULTS: In both groups, carriers of CYP2C19*2 and *3 mutant alleles showed significantly reduced platelet inhibition compared with non-carriers (Table). All other polymorphism had no influence on response to clopidogrel. The rate of HPPR was 5.0% in the triple group and 21.4% in the high-MD group (p < 0.001). To identify the predictors of HPPR in the high-MD group, we performed multivariate analyses including variables with p value < 0.2 in univariate analyses for the HPPR vs. non-HPPR groups. Carriage of CYP2C19*2 and *3 mutant alleles was the only predictor of HPPR (odds ratio 4.292, 95% confidence interval 1.330 to 13.889, p = 0.015).
CONCLUSIONS: Although platelet response to triple antiplatelet therapy is affected by CYP2C19 polymorphism, it inhibits platelet aggregation sufficiently. In carriers of CYP2C19 mutant allele, high-MD clopidogrel therapy can not achieve adequate platelet inhibition.
PRmax = maximal platelet reactivity; PRlate = late platelet reactivity;
wild type = CYP2C19*1/*1
|