Background: No-reflow phenomenon is a serious complication of percutnaneous coronary intervention (PCI) and associated with poor prognosis. We evaluated triple antiplatetet therapy could improve clinical outcomes in patients with acute myocardial infarction (MI) who had no-reflow phenomenon during PCI compared with dual antiplatelet therapy.
Methods: 371 eligible patients who were enrolled in Korean Acute MI Registry (KAMIR) and had no-reflow phenomenon during PCI, were followed up at least 1year. They received either dual antiplatelet therapy (aspirin and clopidogrel, group I, n=271) or triple antiplatetlet therapy (aspirin, clopidogrel, and cilostazol, group II, n=100). Angiographic no-reflow phenomenon was defined as post-PCI TIMI flow grade 0,1 and 2.
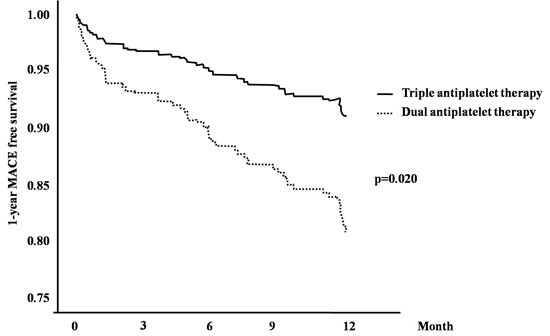
Results: Clinical characteristics of both groups were similar except that group I was older and had higher serum level of C-reactive protein. Angiographic characteristics were comparable between the groups except that group II received more stents (1.3±0.6 vs. 1.6±0.8, p=0.004). At 1 month, death and the composite of major adverse cardiac events (MACEs) were not different. At 6 month, MI and target lesion revascularization (TLR) were not different. However, the incidence of death (6.3 % vs. 1.0 %, p=0.036) and total MACEs (17.6 % vs. 7.2 %, p=0.014) were lower in group II. At 12 month, the incidence of death (7.0 % vs. 4.0 %, p=0.286), TLR (2.2 % vs. 3.0 %, p=0.674) were not different. But total MACEs were lower in group II (22.1 % vs. 14.0 %, p=0.038). Triple antiplatelet therapy (OR=0.41, 95%CI: 0.19-0.87, p=0.020) was the independent prognostic factor of 1-year MACEs as well as diabetes (OR=2.19, 95%CI: 1.19-4.04, p=0.012), Killip class III/IV (OR=1.97, 95% CI:1.09-3.55, p=0.025).
Conclusion: Triple antiplatelet therapy is superior to reducing major adverse cardiac events in patients with acute MI who had no-reflow phenomenon during PCI compared with dual antiplatelet therapy.
|