이달의 증례
- 페이지 경로
- HOME > 자료실 > 이달의 증례



|
이달의 중재술 / 2018년 6월 Successful Provisional T-stenting for Left Main Bifurcation Lesion in Patients with Acute Myocardial Infarction |
|||||||||||||||||||||||||||||
| 저자 | Jumin Won, MD, Min Chul Kim, MD, PhD, Doo Sun Sim, MD, PhD, Young Joon Hong, MD, PhD, Ju Han Kim, MD, PhD, YoungkeunAhn, MD, PhD, FACC, FSCAI and Myung Ho Jeong MD, PhD, FACC, FAHA, FESC, FSCAI | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 소속 | The Heart Center of Chonnam National University Hospital | ||||||||||||||||||||||||||||
|
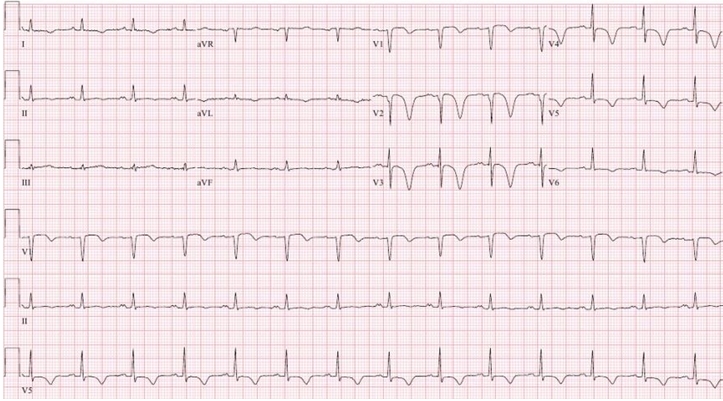
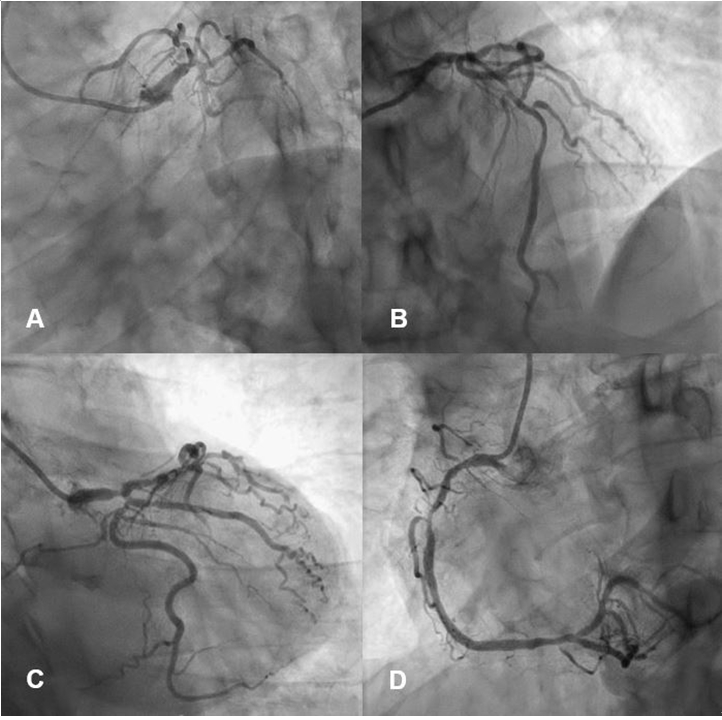
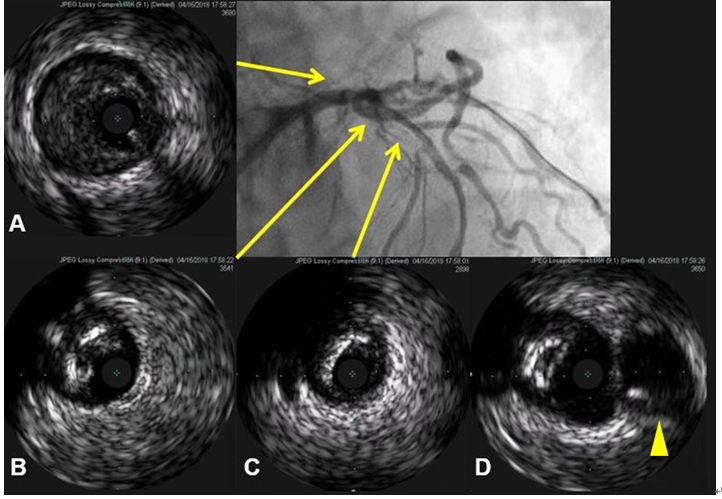
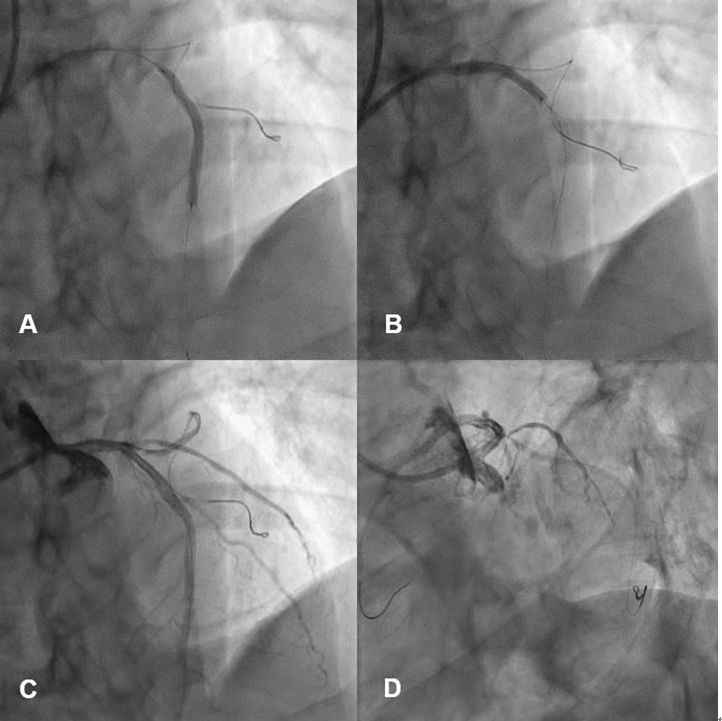
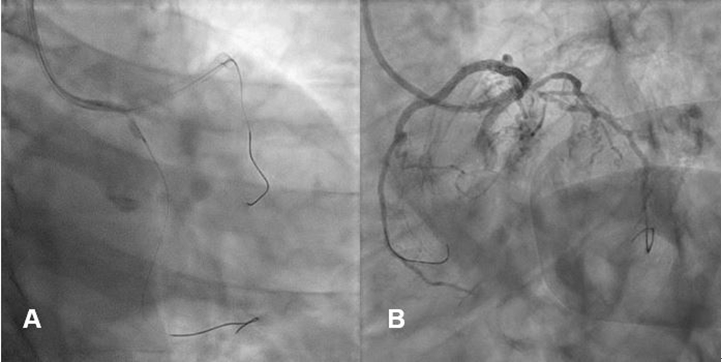
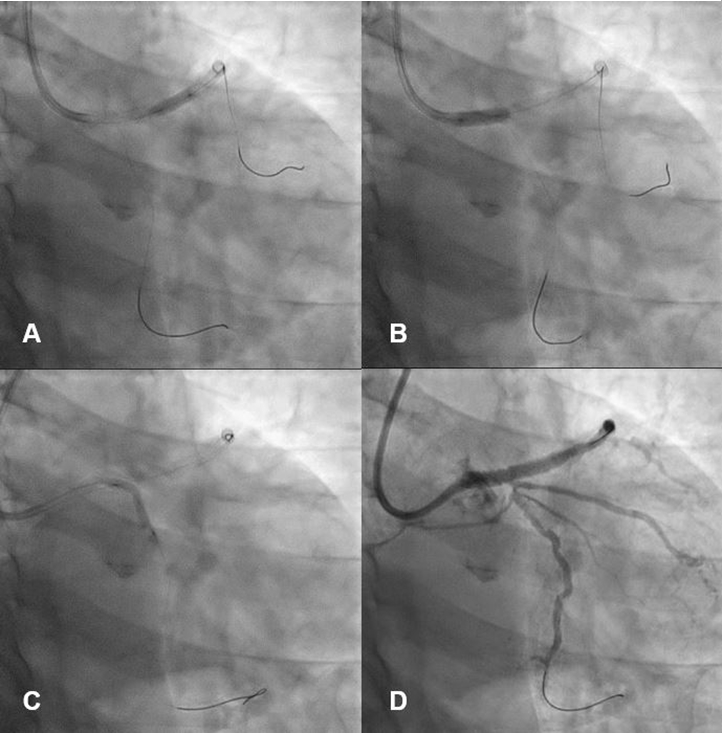
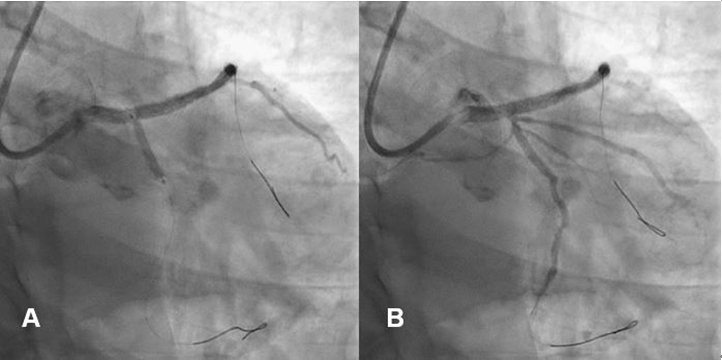
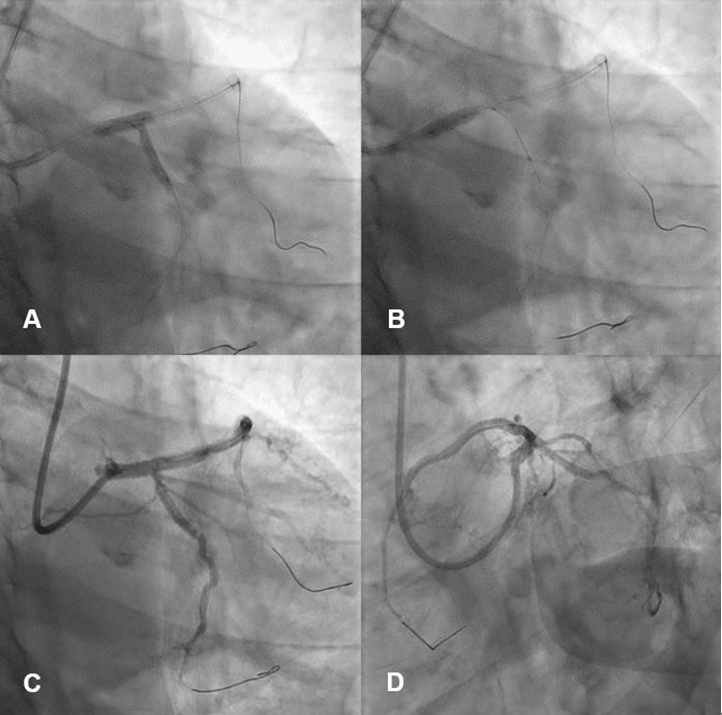
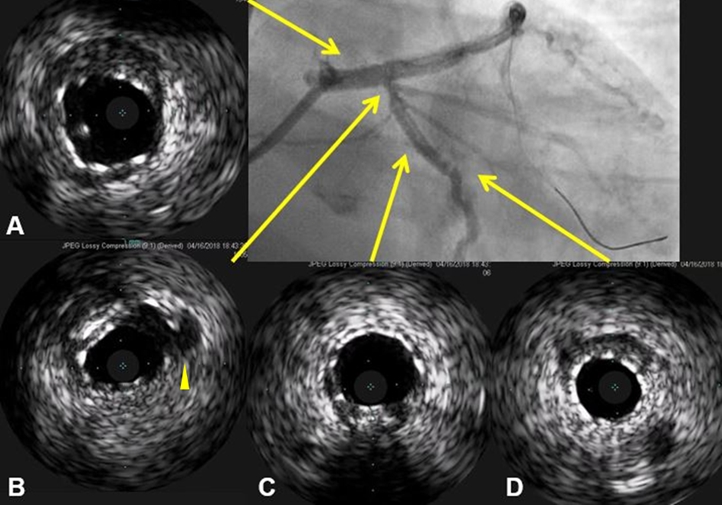
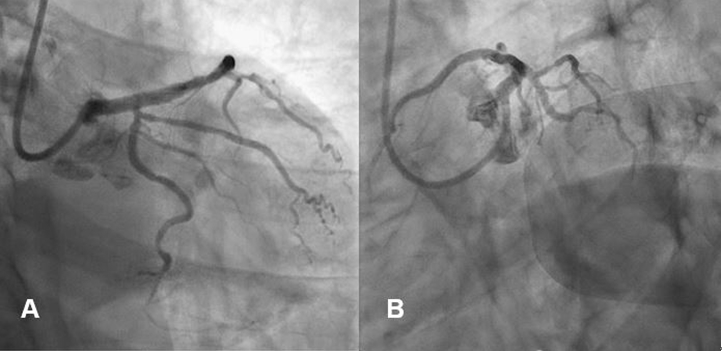
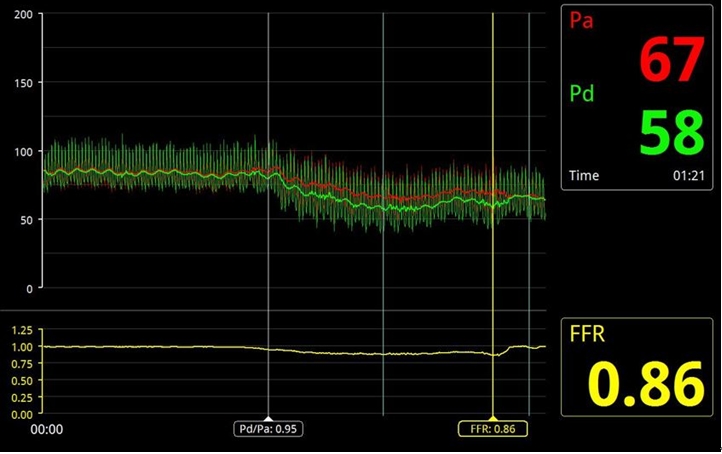
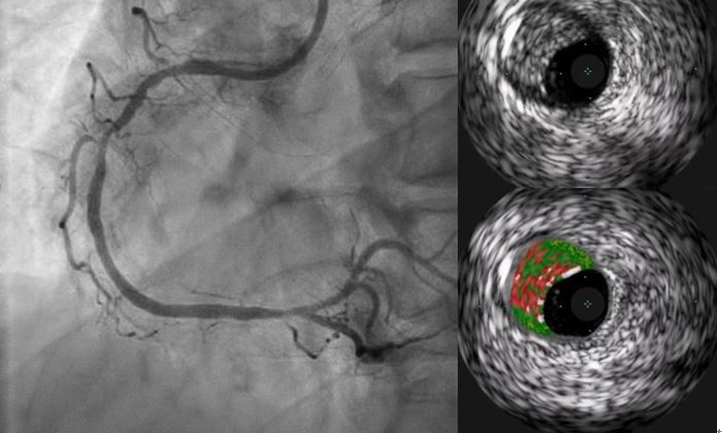
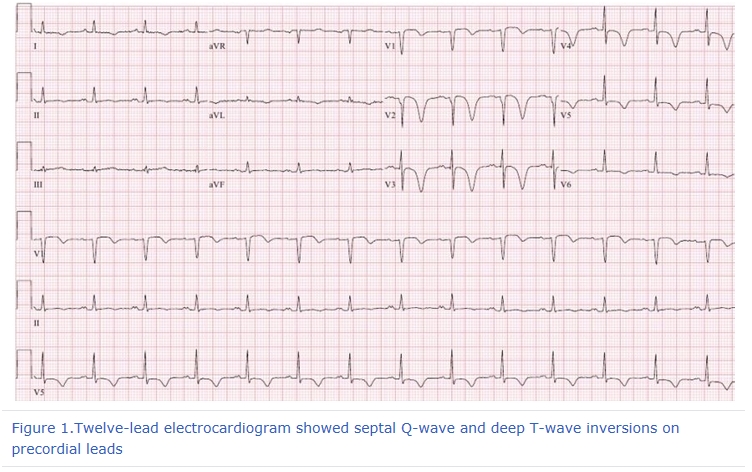
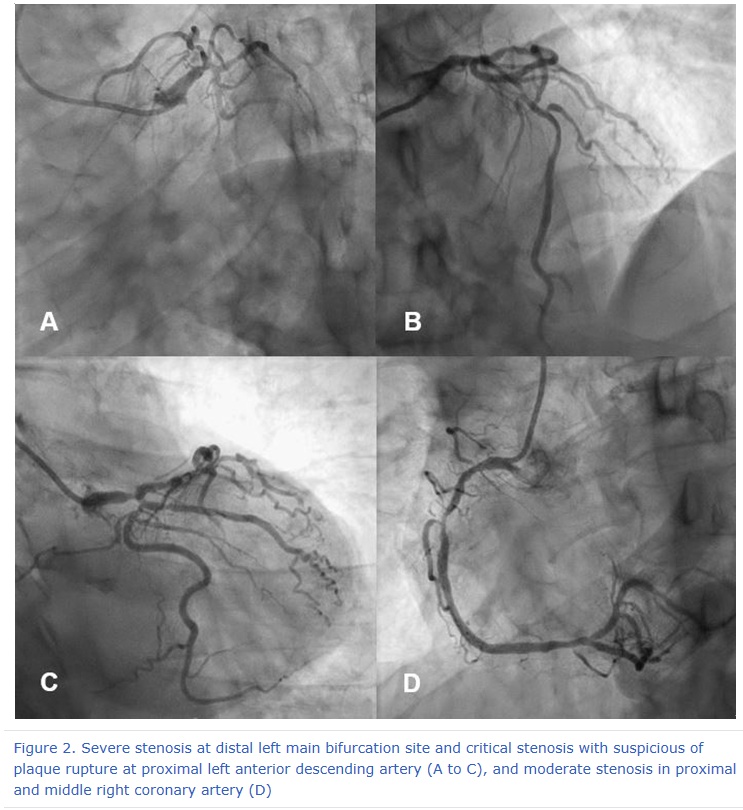
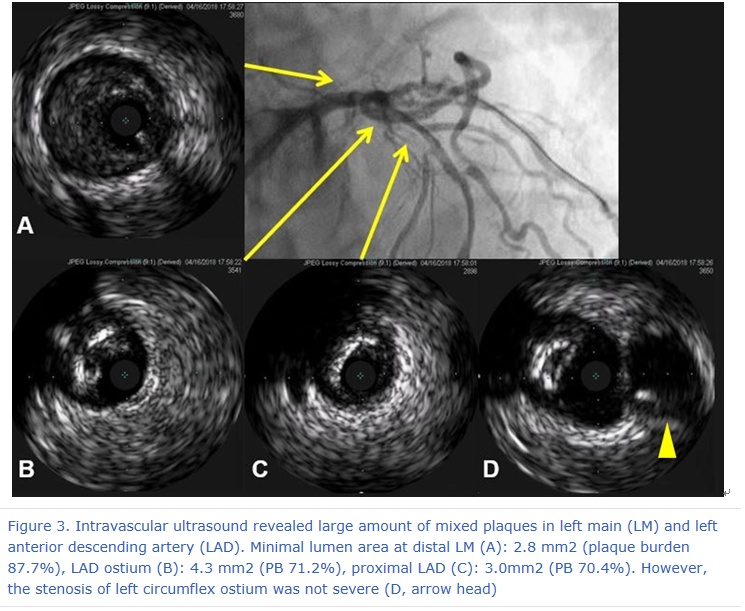
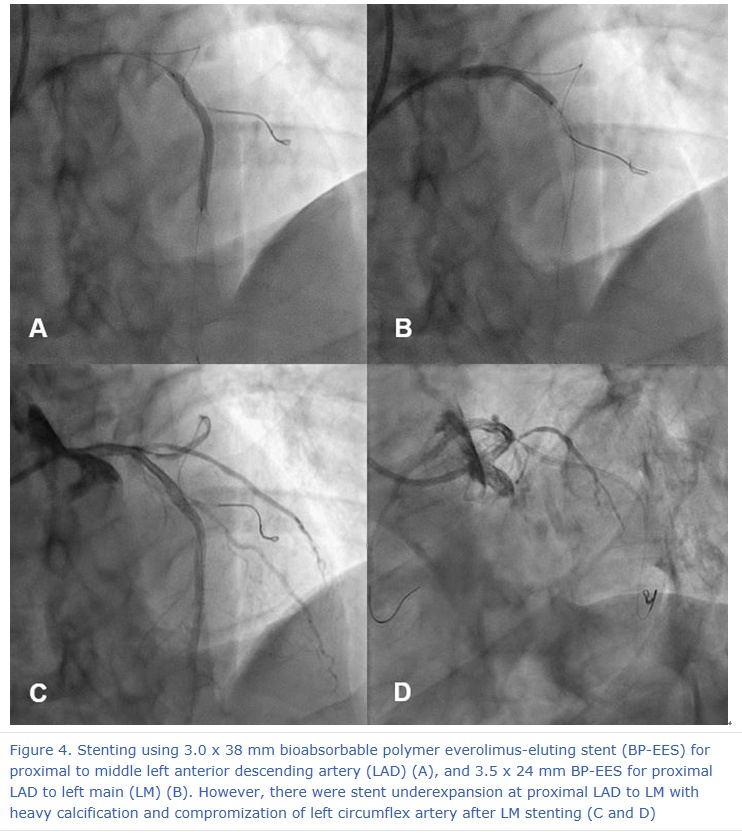
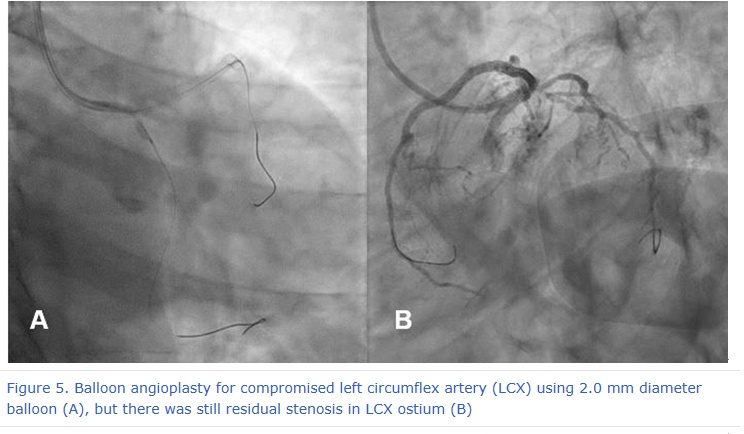
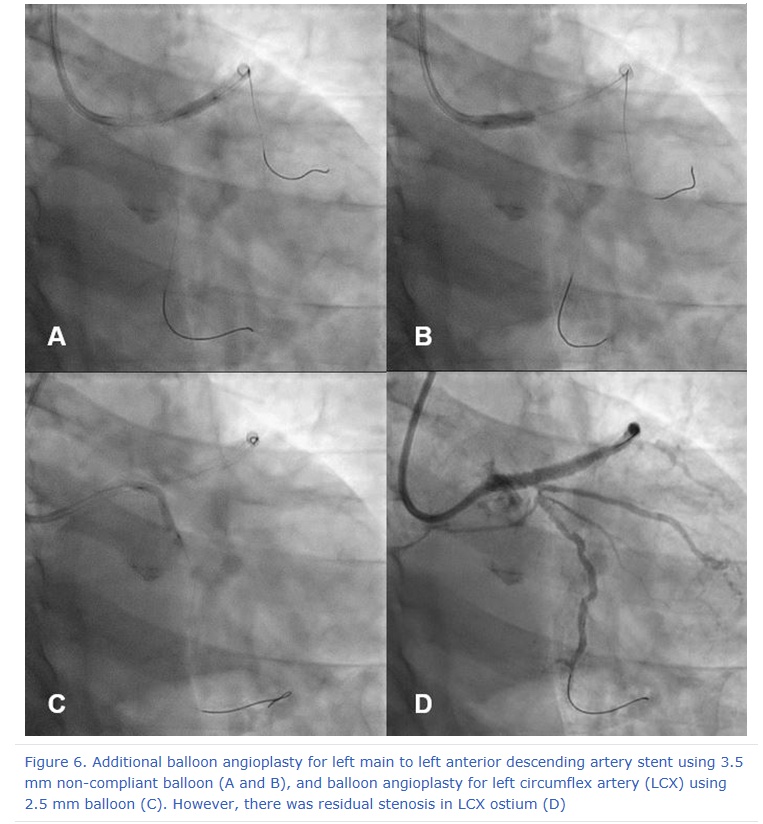
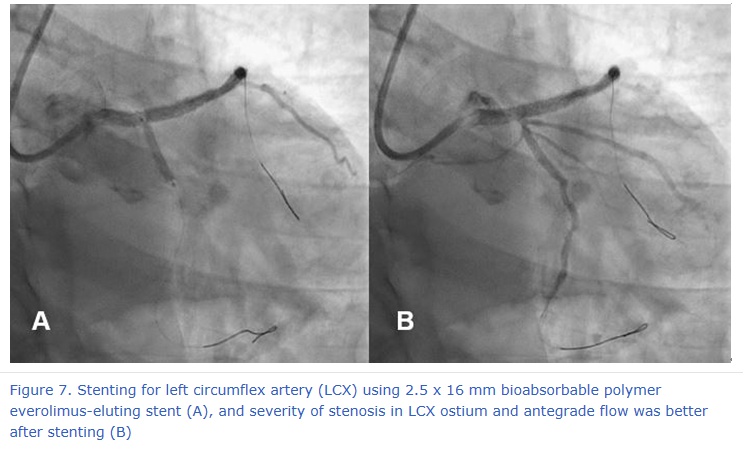
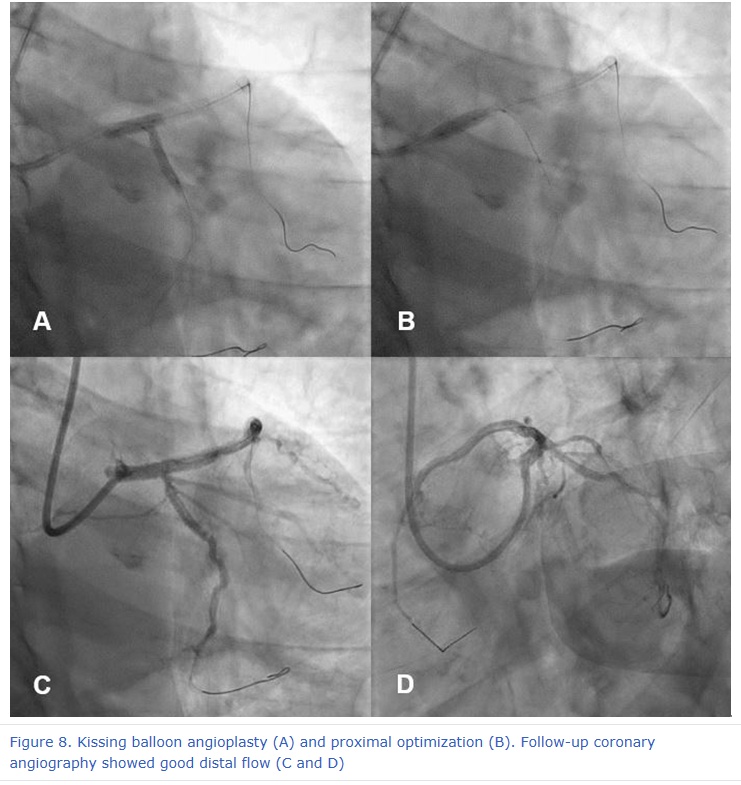
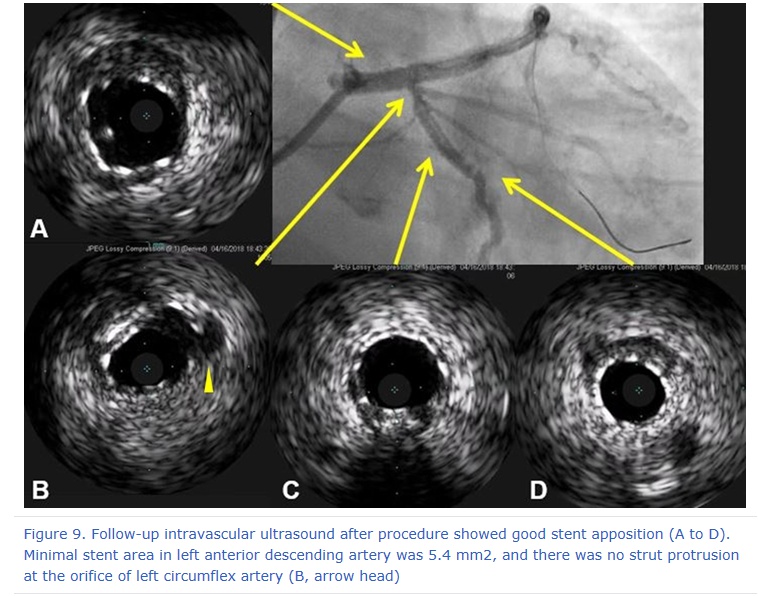
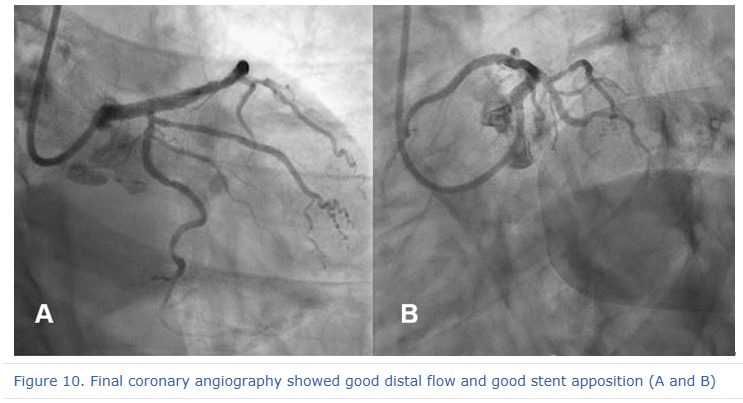
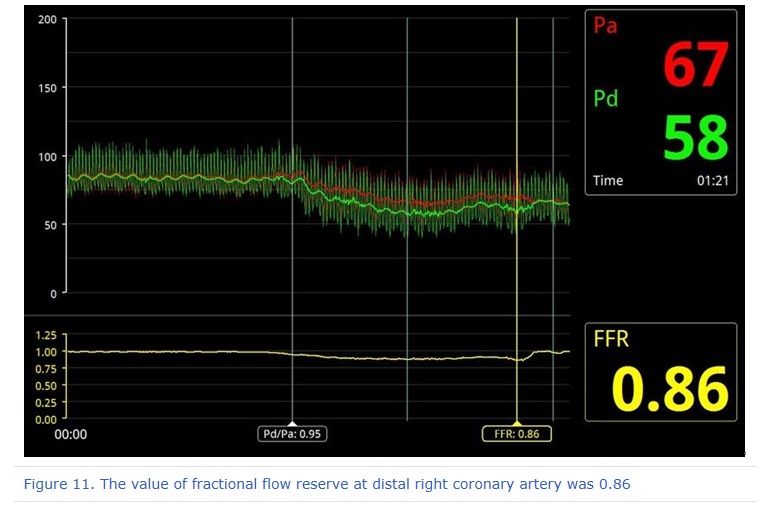
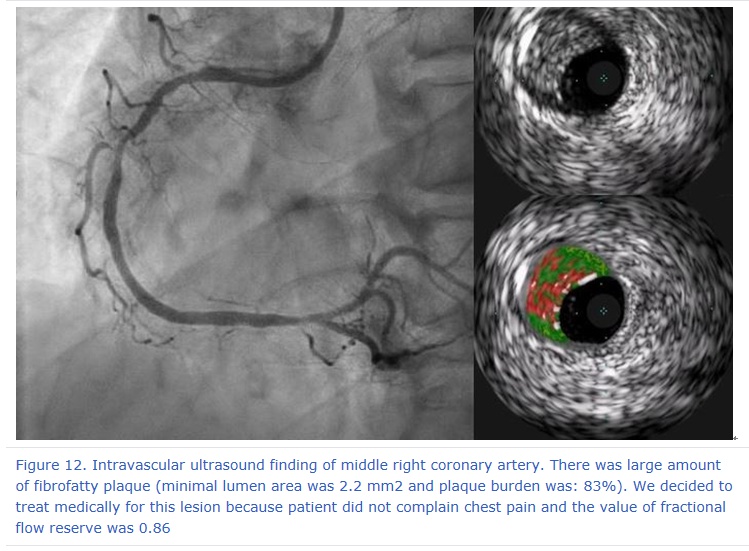
A 61-year-old man was admitted to emergency department of Chonnam National University Hospital for severe chest pain. He suffered from new onset severe angina a day ago. It was a squeezing nature. He was a 30-pack-year current smoker. Twelve-lead electrocardiogram (ECG) showed septal Q-wave, and T-wave inversions on precordial leads (Figure 1). Transthoracic echocardiography showed hypokinesia in left anterior descending artery (LAD) territory with mild decreased left ventricular systolic function (left ventricular ejection fraction 48%). The level of cardiac enzyme was elevated (troponin-I 3.70 ng/ml [reference 0-0.05]), therefore, we took early invasive strategy for non-ST elevation myocardial infarction. On coronary angiography (CAG), there was severe stenosis at distal left main (LM) bifurcation site and critical stenosis with suspicious of plaque rupture at proximal LAD. There was moderate stenosis in proximal and middle right coronary artery (RCA) (Figure 2). After balloon angioplasty using 2.0 mm diameter balloon for proximal LAD, we did intravascular ultrasound (IVUS) for LAD to LM to evaluate plaque characteristics and severities. IVUS revealed a large amount of mixed plaque in distal LM, LAD ostium and proximal LAD. The minimal lumen area (MLA) was 2.8 mm2 at distal LM, 4.3 mm2 at LAD ostium and 3.0 mm2 at proximal LAD. We planned to do provisional stent implantation for distal LM to middle LAD because the stenosis at LCX ostium was not severe in IVUS (Figure 3). Firstly, we implanted 3.0 x 38 mm biodegradable polymer everolimus-eluting stent (BP-EES, Synergy™, Boston Scientific, MA, US) for proximal to middle LAD, and 3.5 x 24 mm BP-EES (Synergy™, Boston Scientific, MA, US) for proximal LAD to LM. After proximal optimization technique (POT), follow-up CAG showed stent underexpansion at proximal LAD to distal LM with heavy calcification, and compromised LCX and median branch with TIMI II antegrade flow (Figure 4). Patient complained severe chest pain and blood pressure was dropped, therefore, we immediately reinserted the wire in LAD across the strut of LAD stent into LCX and did balloon angioplasty for LCX using 2.0 mm diameter balloon. After that, the antegrade flow in LCX was better, but there was still residual stenosis in LCX ostium (Figure 5). So, we changed the plan and took provisional two stent strategy. Firstly, we did additional balloon angioplasty for LM to LAD stent using 3.5 mm non-compliant balloon. Secondly, balloon angioplasty again for LCX using 2.5 mm diameter balloon (Figure 6). And then, we implanted 2.5 x 16 mm BP-EES (Synergy™, Boston Scientific, MA, US) for LCX (Figure 7). Finally, we did kissing balloon angioplasty and POT. Follow-up CAG showed good distal flow (Figure 8). We did IVUS again to evaluate stent optimization which showed good stent apposition and the minimal stent area (MSA) was 5.4 mm2, and there was no strut protrusion at the orifice of LCX (Figure 9). Final CAG also showed good distal flow and good stent apposition (Figure 10). At the fourth hospital day, we did follow-up CAG which showed good distal flow and stent apposition in left coronary artery, and still moderate stenosis in proximal and middle RCA. We did fractional flow reserve (FFR) first and the value of it was 0.86 (Figure 11). We also examined IVUS for evaluation of plaque characteristic which showed large amount of fibrofatty plaque, the MLA was 2.2 mm2 and plaque burden was 83% (Figure 12). We deferred stent implantation and treated this lesion medically because patient did not complain chest pain and the value of FFR was 0.86. He discharged at the fifth hospital day without any in-hospital adverse events. Coronary bifurcation lesion remains one of the most fascinating and challenging lesion subsets with lower procedural success rate and increased rates of long term adverse cardiac events. In drug-eluting stent era, the simpler is the better. Although we successfully performed provisional 2-stenting for LM bifurcation lesion, provisional stenting technique with proximal optimization technique is better than elective 2-stent technique, except true bifurcation lesion and/or high risk of occlusion (Sawaya FJ et al. JACC Cardiovasc Interv 2016;9:1861-78).
|
|||||||||||||||||||||||||||||
| 첨부파일1 | |||||||||||||||||||||||||||||

- Tel 02-3275-5258
- Fax 02-3275-5259
- E-mail herz1@circulation.or.kr
- Copyright© The Korean Society of Cardiology


- 심장학 최신지견 따라잡기
- 진료지침

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}