이달의 증례
- 페이지 경로
- HOME > 자료실 > 이달의 증례



|
이달의 중재술 / 2018년 6월 The angiographic neo-carina formed by neointimal growth in patients with left main bifurcation lesion treated by V-stent technique 12 years ago. |
|||||||||||
| 저자 | Dongyoung Lee, Je Sang Kim, Hyun Jong Lee, Ji Park Kim, Young Jin Choi, Tae-Hoon Kim | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 소속 | Sejong General Hospital | ||||||||||
|
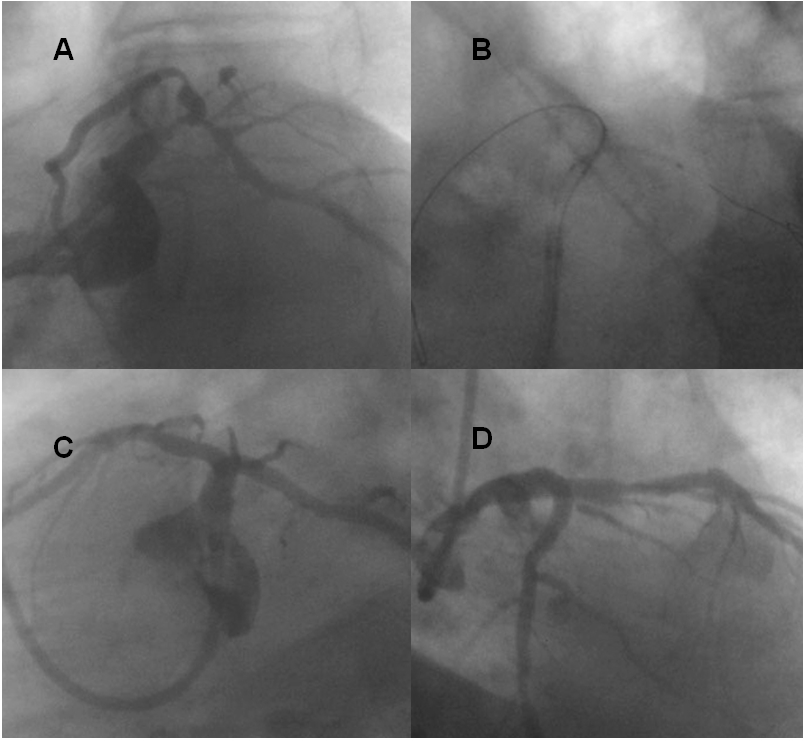
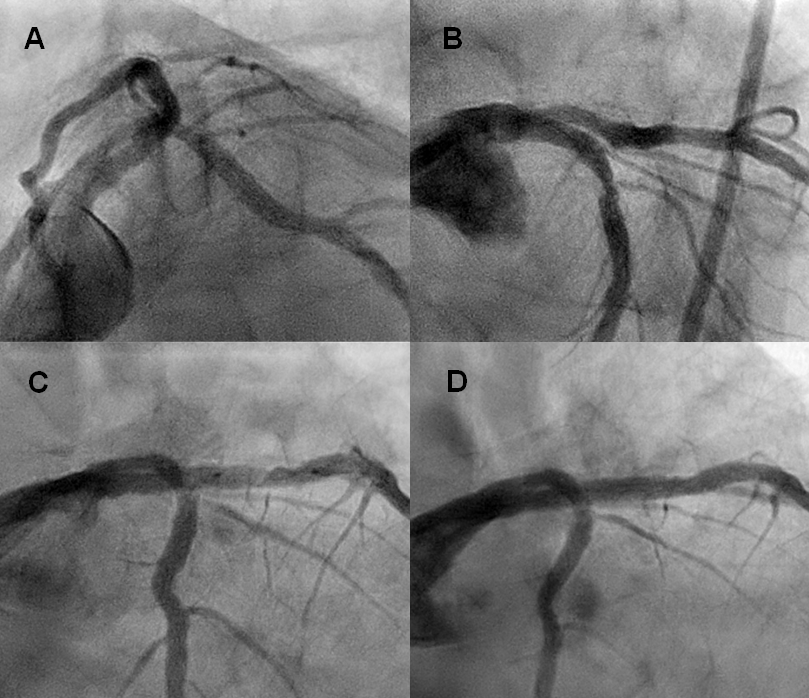
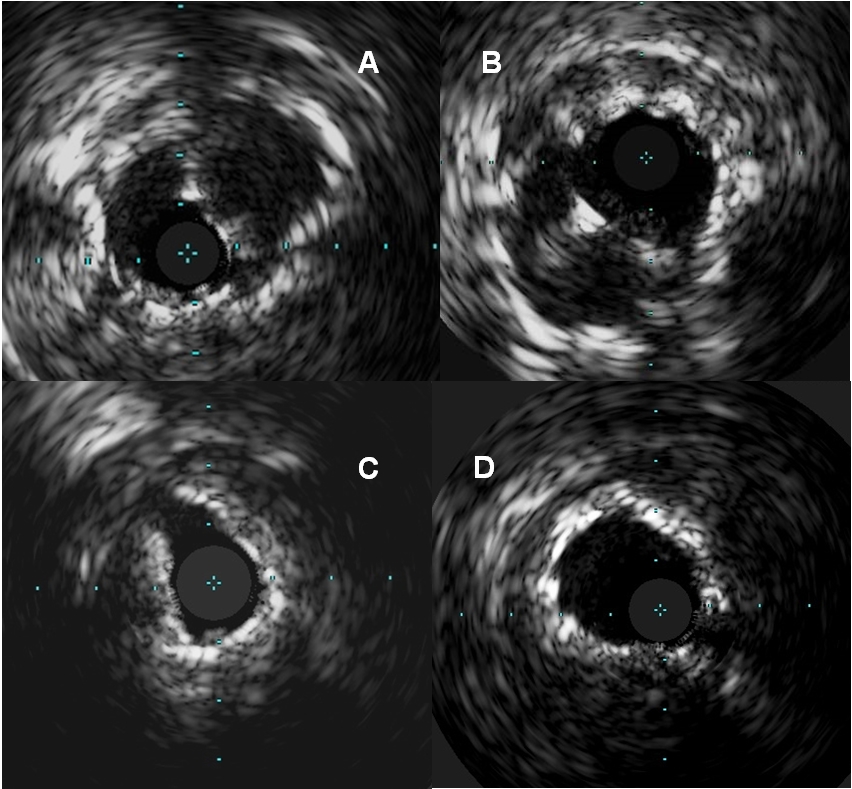
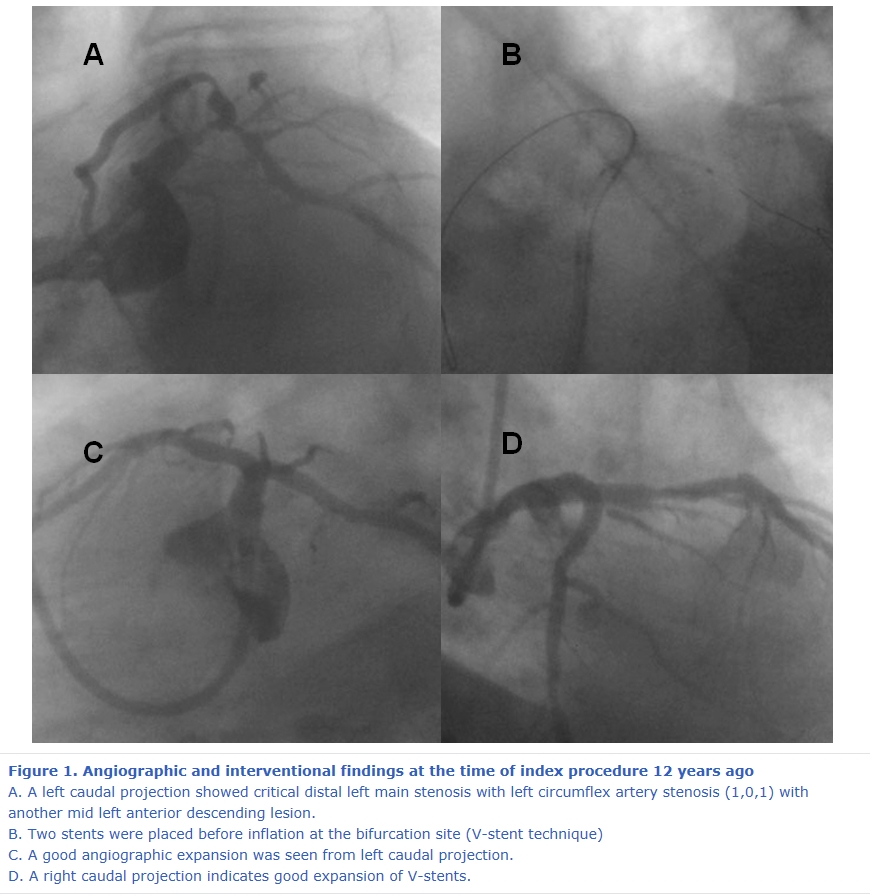
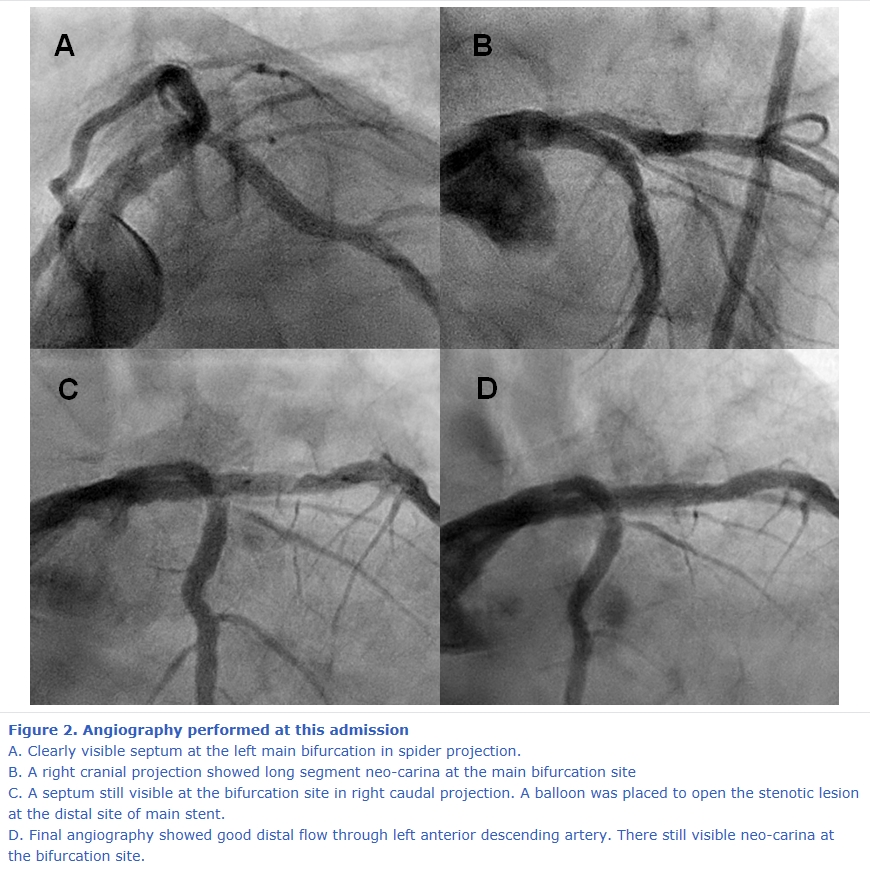
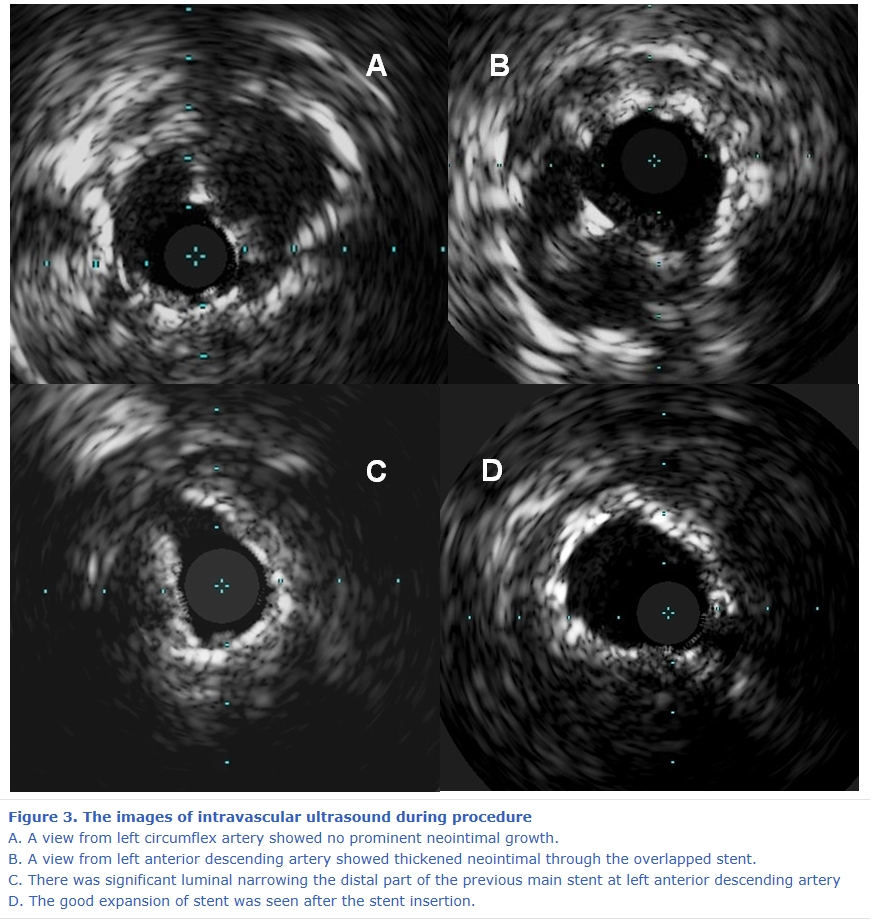
A 77-year-old male patient visited our hospital with CCS (Canadian Cardiovascular Society) grade 1 exertional chest pain. He underwent percutaneous coronary intervention (PCI) for unstable angina using two Taxus stents at the left main bifurcation by V-stent technique 12 years ago (3.0 x 15mm to the LAD and 3.0 x 18 to the LCX, Fig 1). At that time the other stent was deployed separately to the mid LAD ( 3.0 x15 mm bare metal stent). His current medications were anti-hypertensive medications and the single antiplatelet agent (100mg of aspirin) without statin. A treadmill test showed significant horizontal ST segment depression during stage 2 and recovery phase, so elective coronary angiography was planned. To our surprise, there was an angiographically visible neo-carina in the overlapped part of main stents at the left main bifurcation (Fig 2). It was not existed at the time of stents deployment (Fig1C and 1D). An intravascular ultrasonography (IVUS) also confirmed 0.3mm of neo-intima at the flow divider side of overlapped part V-stents dominantly seen from the LAD side (Fig 3A and 3B). Fortunately, enough lumen area was secured from the LAD and LCX bifurcation sites. The main cause of the anginal pain seemed from the large amount of eccentric plaque at the proximal LAD, which was grown at the distal part of main stent (minimal lumen area [MLA] 2.6 mm2; Fig. 2B and 3C). After balloon angioplasty (Fig 2C), we implanted 3.0 x 22 mm everolimus-eluting stent (Onyx®) between the previously deployed stents at the left main and the mid LAD (Fig 2D) and good stent expansion was seen from post stent IVUS (Fig 3D). His symptom was gone after the procedure. Although, PCI was considered as alternative viable treatment strategy to coronary artery bypass grafting for left main coronary disease1, late worrisome outcome could be expected to the patients treated by complex stenting especially for 1st generation stent. Similarly, diverse two stent technique for left main bifurcation was introduced according to the various lesion morphology however, outcomes from each technique were not clearly revealed. Y or V-stent technique was limitedly used when there is the large size discrepancy between the left main and the LAD or LCX. A possible limitation for this technique may be the presence of large part of unopposed struts even after the stent deployment. Moreover, intimal coverage of unopposed struts or proper requirement of duration of dual antiplatelet therapy was not fully studied. Our case showed newly formed septum at the overlapped stents area 12 years after the stent deployment. Recent OCT based bifurcation study indicated that the thickness of neointimal hyperplasia was higher only at the proximal edge of LAD and LCX ostium.2 Unlikely to this study, our patients had very long and thick neointimal growth through the nearly entire overlapped stent at the bifurcation. It is hard to guess when the patient had this unique neointimal growth at the bifurcation site, because he only underwent angiography at the time of index PCI. Although there was chance to have gradual intimal growth through the years, previous long-term (≥2 years) OCT data for 1st generation DES showed that there was no great thickness difference between 9-month and 2-year follow up in Taxus stent implantation.3 Although the proper explanation for this neointimal growth was not enable, this interesting case showed new carina through the overlapping stent with modest neointimal growth without making vessel occlusion.
Reference
|
|||||||||||
| 첨부파일1 | |||||||||||

- Tel 02-3275-5258
- Fax 02-3275-5259
- E-mail herz1@circulation.or.kr
- Copyright© The Korean Society of Cardiology


- 심장학 최신지견 따라잡기
- 진료지침

{kind=link}
{kind=link}
{kind=link}