A 78 year-old male visited the outpatient department of Chonnam National University Hospital with intermittent chest pain for 4 months. He underwent percutaneous coronary intervention (PCI) for acute myocardial infarction (AMI) using bare metal stent in the proximal right coronary artery (RCA) 8 years ago. After that, he had undergone repeat intervention using drug eluting ballooning 7 years ago and PCI for mid RCA 6 years ago due to repeated in-stent restenosis (ISR) in RCA. He was treated with dual anti-platelet therapy of aspirin (100 mg daily) and clopidogrel (75 mg daily). Recently, he suffered from chest pain intermittently and was taken to our hospital. The 12-lead electrocardiogram showed normal sinus rhythm and left bundle branch block (no interval change) (Figure 1), and the level of cardiac enzymes were within normal range. He underwent elective coronary angiography (CAG), and it revealed chronic total occlusion in proximal RCA (Type IV ISR) (Figure 2A) with moderate stenosis in proximal left descending artery (LAD). We considered to do staged PCI for proximal LAD. After wiring into RCA with microcatheter backup, stepwise ballooning using 1.5 mm and 2.5 mm diameter balloon was done. Then, a 3.5 x 38 mm everolimus-eluting stent (Xience Alpine®) was implanted at proximal RCA (Figure 2B). Just after stenting with up to 10 atmospheres, no reflow below the lesion site was shown on follow-up CAG (Figure 2C). Coronary blood flow was not restored after intracoronary adenosine, nicorandil and glycoprotein IIb/IIIa inhibitor bolus injection in RCA (Figure 2D). Although we did additional ballooning from distal to proximal RCA again and again (Figure 3A), follow-up CAG showed still no reflow in RCA (Figure 3B). So, we infused intracoronary adenosine and nicoradil using microcatheter from proximal to distal RCA selectively (Figure 3C). Final CAG showed improved antegrade flow (TIMI III) in RCA without significant residual stenosis (Figure 3D). He was transferred to coronary care unit and monitored with anticoagulation for 1 day.
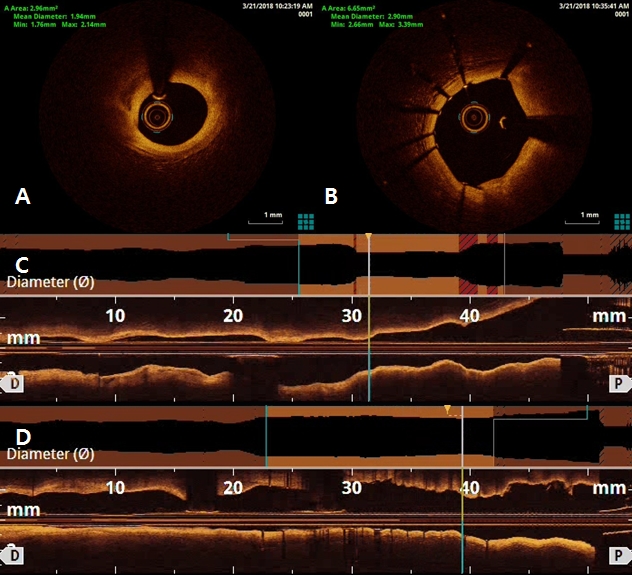
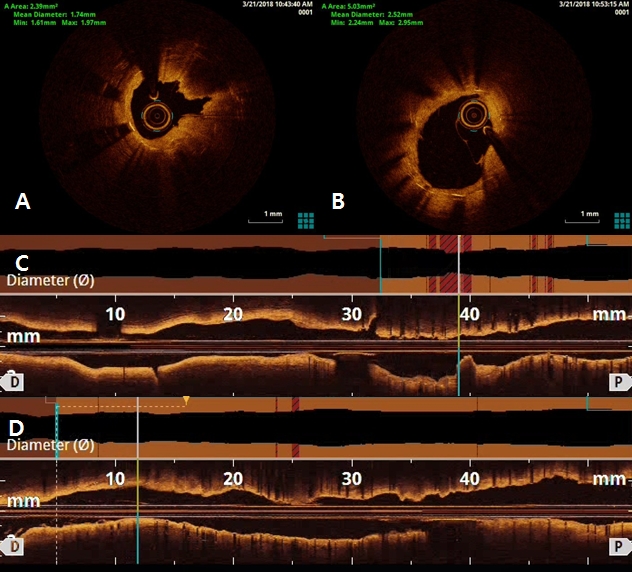
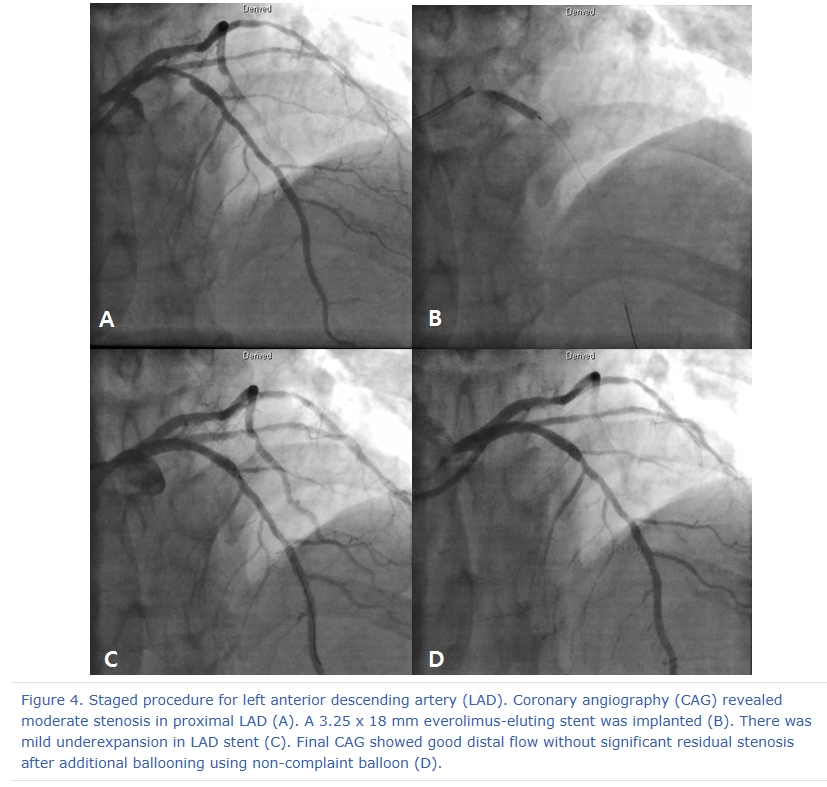
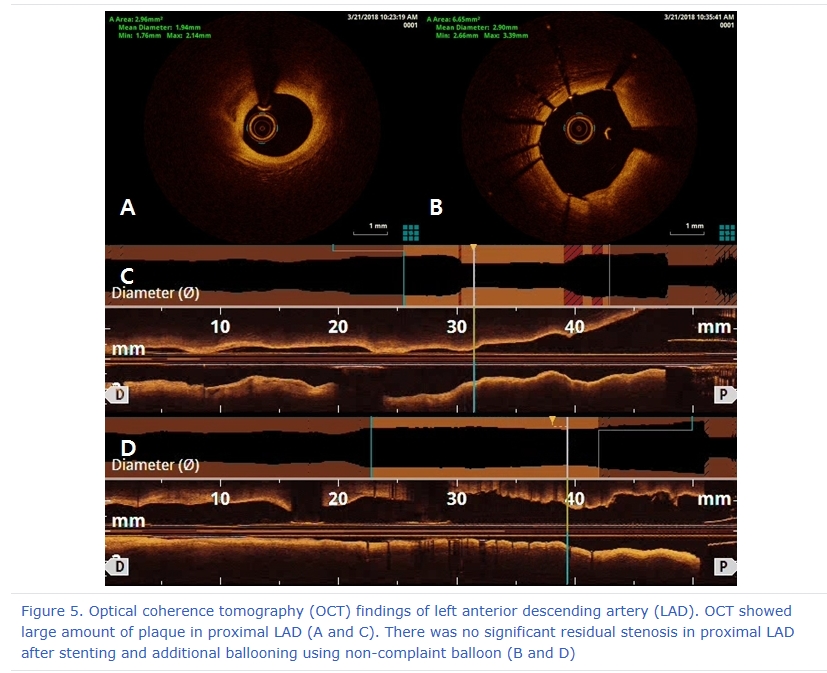
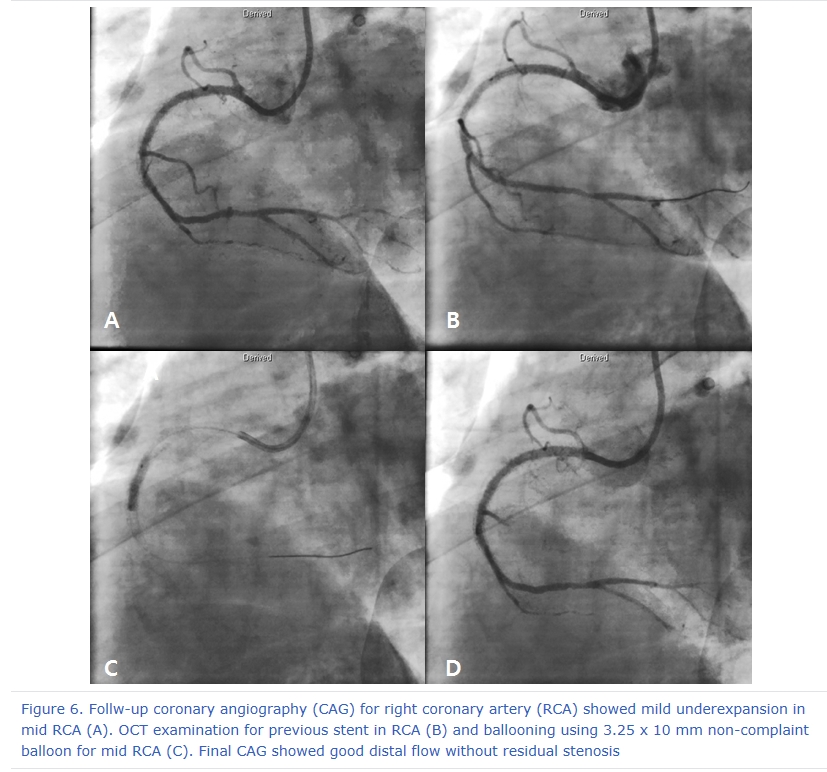
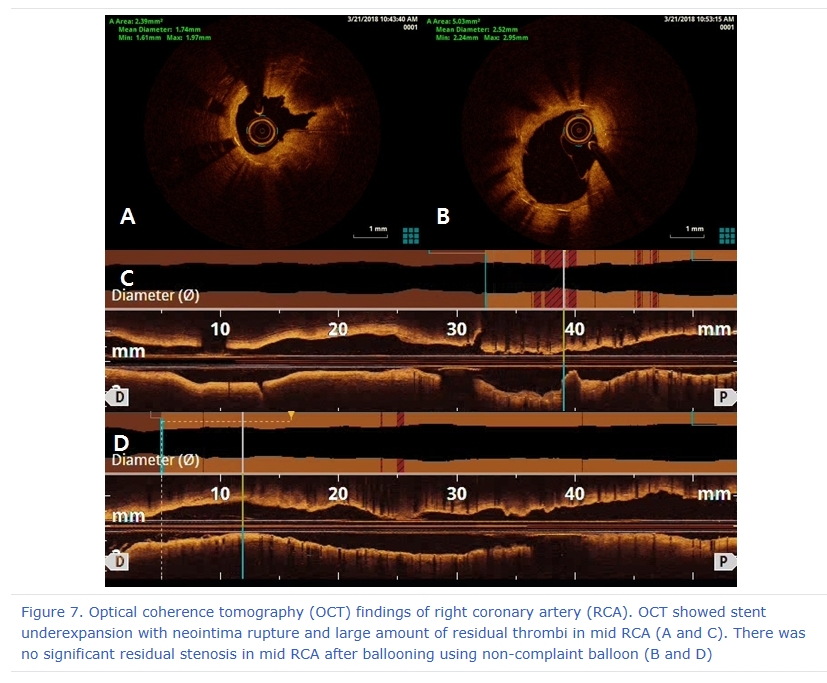
After 3 days later, we performed 2nd stage PCI for proximal LAD. CAG reveled moderate stenosis in proximal LAD (Figure 4A), so we examined optical coherence tomography (OCT) for further evaluation. It showed large amount of plaque (minimal lumen area [MLA] 2.62 mm2) (Figure 5A and 5C). We directly implanted 3.25 and 18 mm everolimus-eluting stent (Xience Alpine®), but follow-up CAG showed mild under-expansion, so we did additional ballooning using 3.25 x 10mm non-complaint balloon (Figure 4B and 4C). Follow-up OCT and CAG showed good distal flow without significant residual stenosis. (post-PCI cross sectional area [CSA] 6.65 mm2) (Figure 4D, 5B and 5D). Because of no-reflow phenomenon for RCA in previous PCI, we performed follow-up CAG and OCT for RCA. CAG and OCT showed stent underexpansion with neointima rupture and large amount of residual thrombi in mid RCA (MLA 2.39 mm2) (Figure 6A, 6B, 7A and 7C). So we did ballooning using 3.25 x 10 mm non-complaint balloon for mid RCA (Figure 6C). Follow-up CAG and OCT showed good distal flow without significant residual stenosis. (CSA 5.03 mm2) (Figure 6D, 7B and 7D). He was discharged without any complications.
No-reflow phenomenon is a serious complication after PCI. It is caused by multiple factors including distal atherothrombotic embolization, ischemic injury, reperfusion injury and susceptibility of coronary microcirculation to injury. It is defined as a state of myocardial hypoperfusion in the presence of a patent coronary artery. No-reflow phenomenon should be undoubtedly a negative consequence of the patient's clinical outcome. Persistent no-reflow in patients with AMI who underwent PCI with coronary stents was associated with poor in-hospital outcomes and increased long-term mortality mainly driven by increased cardiac death despite its low incidence. As described above, it is very important to restore no-reflow during PCI in the clinical outcome of the patient when it occurs. Selective infusion of intracoronary adenosine and nicorandil may be a good option for management of persistent no-reflow. Also, OCT showed neointima rupture and large amount of residual thrombi at no-reflow phenomenon coronary lesion in our patient. OCT might play an important role in intravascular pathophysiology of no-reflow phenomenon.
 |
|
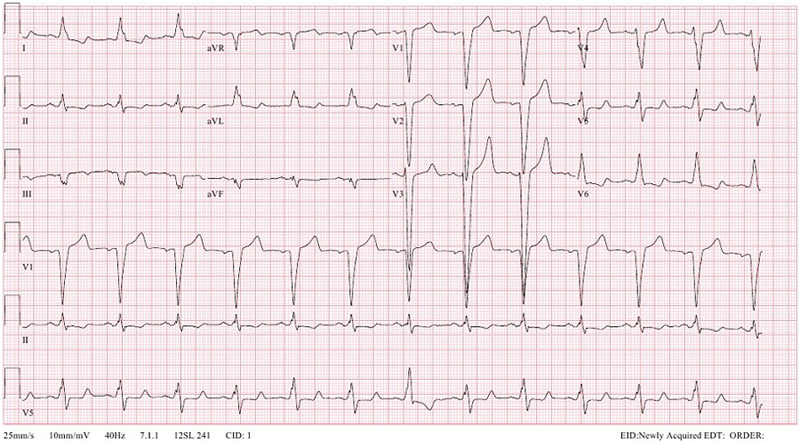
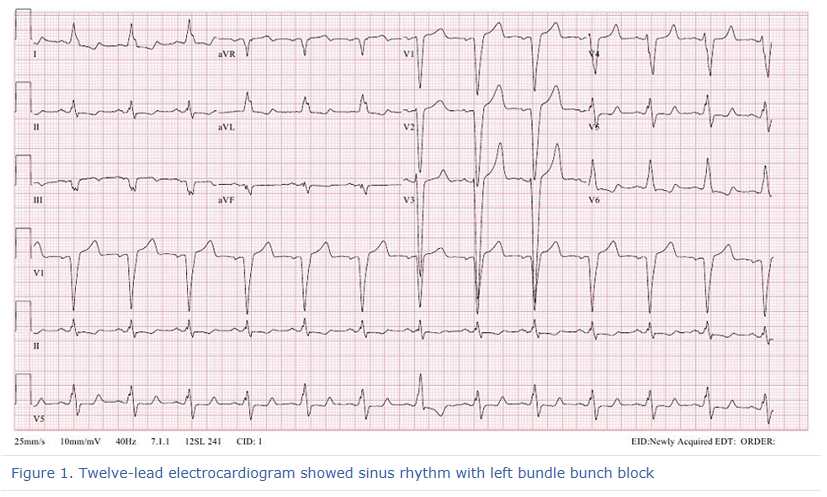
Figure 1. Twelve-lead electrocardiogram showed sinus rhythm with left bundle bunch block
|
 |
|
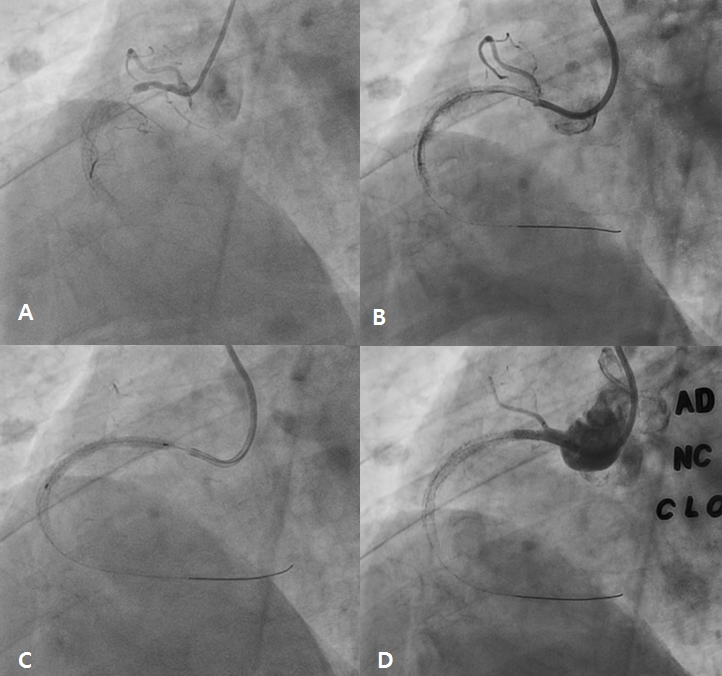
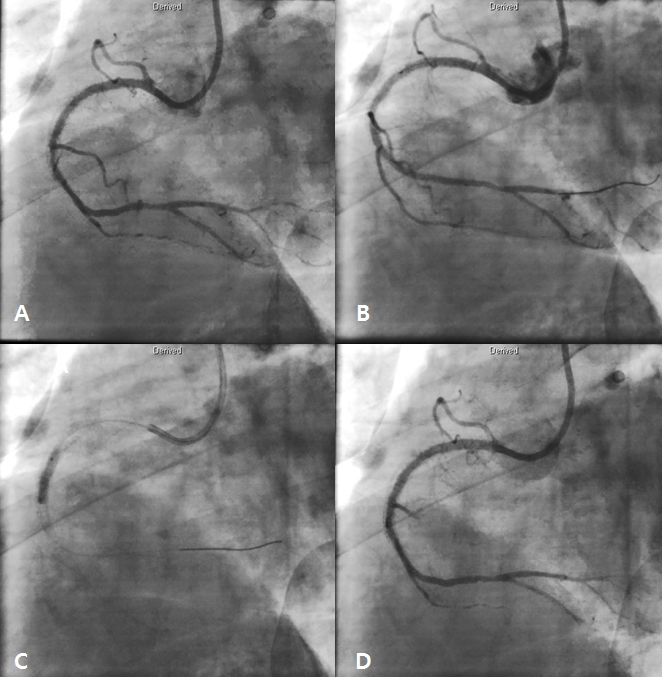
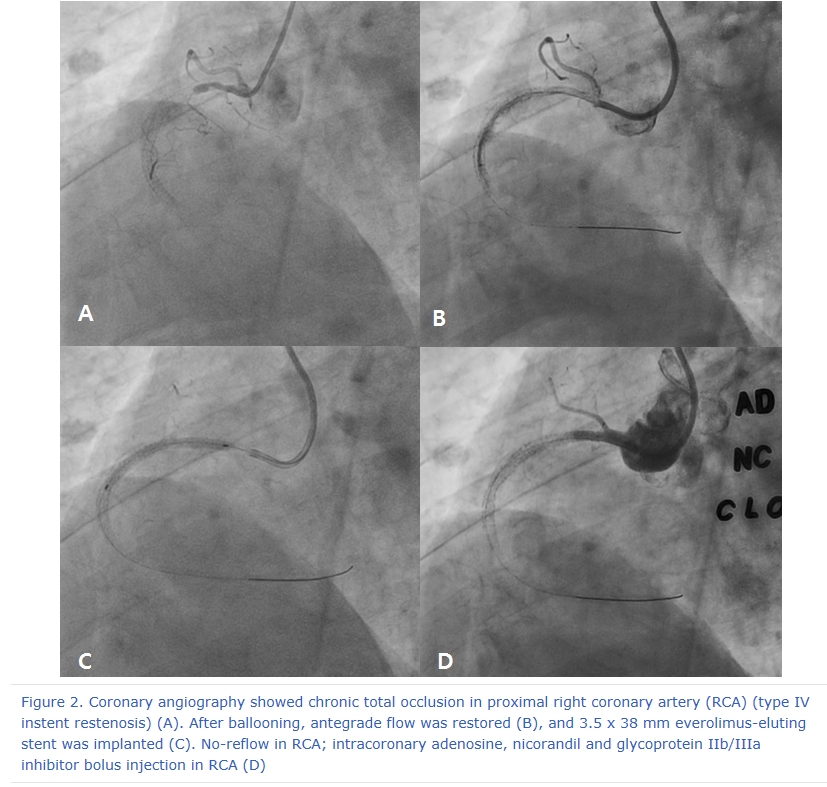
Figure 2. Coronary angiography showed chronic total occlusion in proximal right coronary artery (RCA) (type IV instent restenosis) (A). After ballooning, antegrade flow was restored (B), and 3.5 x 38 mm everolimus-eluting stent was implanted (C). No-reflow in RCA; intracoronary adenosine, nicorandil and glycoprotein IIb/IIIa inhibitor bolus injection in RCA (D)
|
 |
|
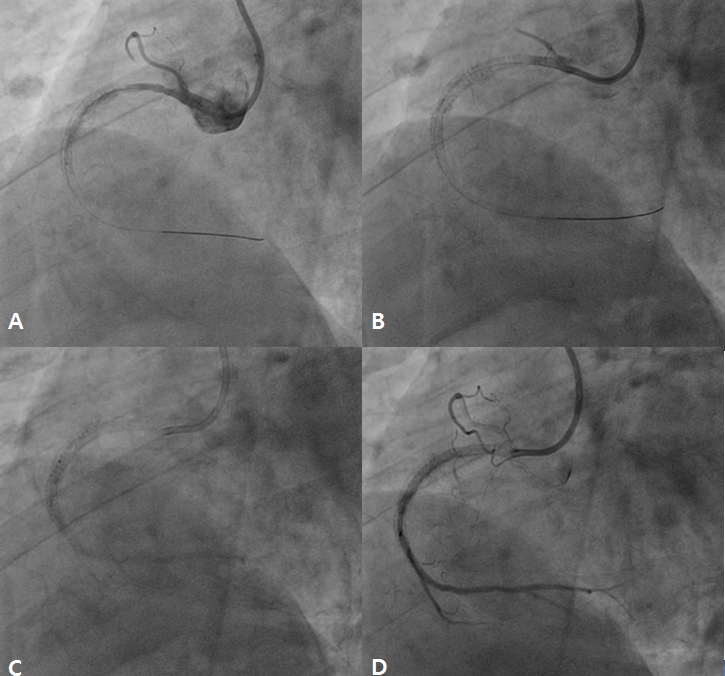
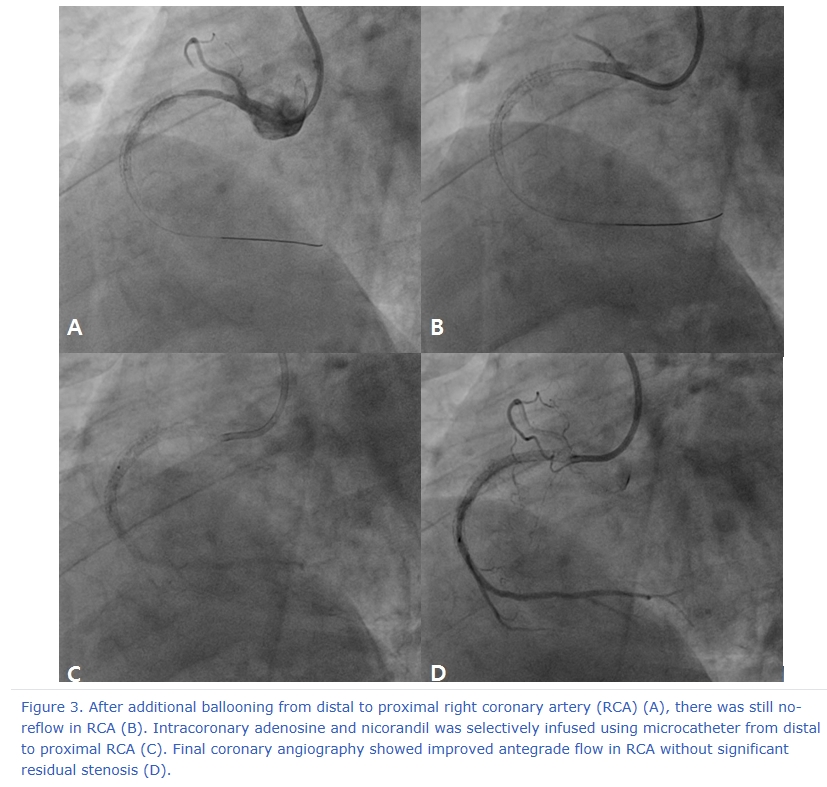
Figure 3. After additional ballooning from distal to proximal right coronary artery (RCA) (A), there was still no-reflow in RCA (B). Intracoronary adenosine and nicorandil was selectively infused using microcatheter from distal to proximal RCA (C). Final coronary angiography showed improved antegrade flow in RCA without significant residual stenosis (D).
|
 |
|
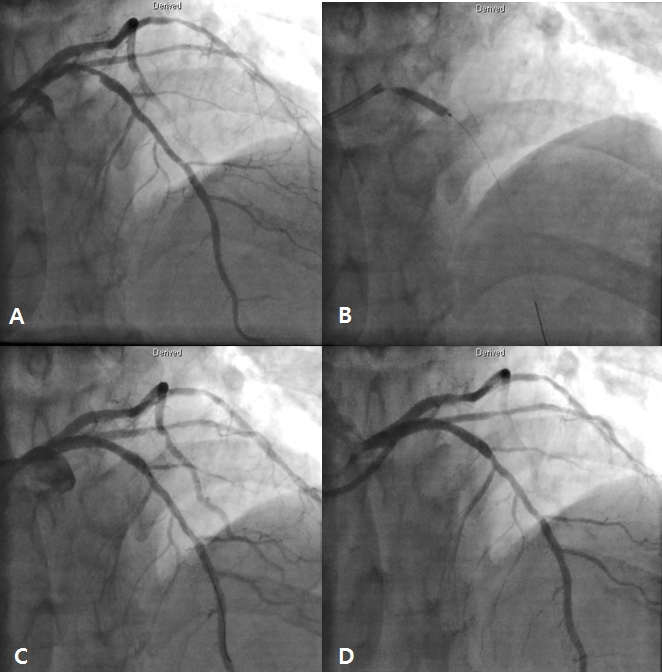
Figure 4. Staged procedure for left anterior descending artery (LAD). Coronary angiography (CAG) revealed moderate stenosis in proximal LAD (A). A 3.25 x 18 mm everolimus-eluting stent was implanted (B). There was mild underexpansion in LAD stent (C). Final CAG showed good distal flow without significant residual stenosis after additional ballooning using non-complaint balloon (D).
|
 |
|
Figure 5. Optical coherence tomography (OCT) findings of left anterior descending artery (LAD). OCT showed large amount of plaque in proximal LAD (A and C). There was no significant residual stenosis in proximal LAD after stenting and additional ballooning using non-complaint balloon (B and D)
|
 |
|
Figure 6. Follw-up coronary angiography (CAG) for right coronary artery (RCA) showed mild underexpansion in mid RCA (A). OCT examination for previous stent in RCA (B) and ballooning using 3.25 x 10 mm non-complaint balloon for mid RCA (C). Final CAG showed good distal flow without residual stenosis
|
 |
|
Figure 7. Optical coherence tomography (OCT) findings of right coronary artery (RCA). OCT showed stent underexpansion with neointima rupture and large amount of residual thrombi in mid RCA (A and C). There was no significant residual stenosis in mid RCA after ballooning using non-complaint balloon (B and D)
|
|







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}