이달의 증례
- 페이지 경로
- HOME > 자료실 > 이달의 증례



|
이달의 영상 / 2018년 2월 Immunoglobulin G4-related Coronary Periarteritis |
|||||||||||||
| 저자 | Hack-Lyoung Kim, Woo-Hyun Lim, Jae-Bin Seo, Woo-Young Chung, Sang-Hyun Kim, Joo-Hee Zo, Myung-A Kim | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 소속 | Division of Cardiology, Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea | ||||||||||||
|
Immunoglobulin G4 (IgG4)-related disease is a recently recognized systemic disorder that is characterized by the infiltration of IgG4-positive plasma cells with fibrosclerosis and elevated serum IgG4 concentration. Although it has been reported that IgG4-related disease can involve in various organs, most of which are glandular or ductal tissues, documents describing coronary artery involvement are relatively rare. In the current report, we present a case of Korean elderly women with clinically diagnosed with IgG4-related coronary arteritis.
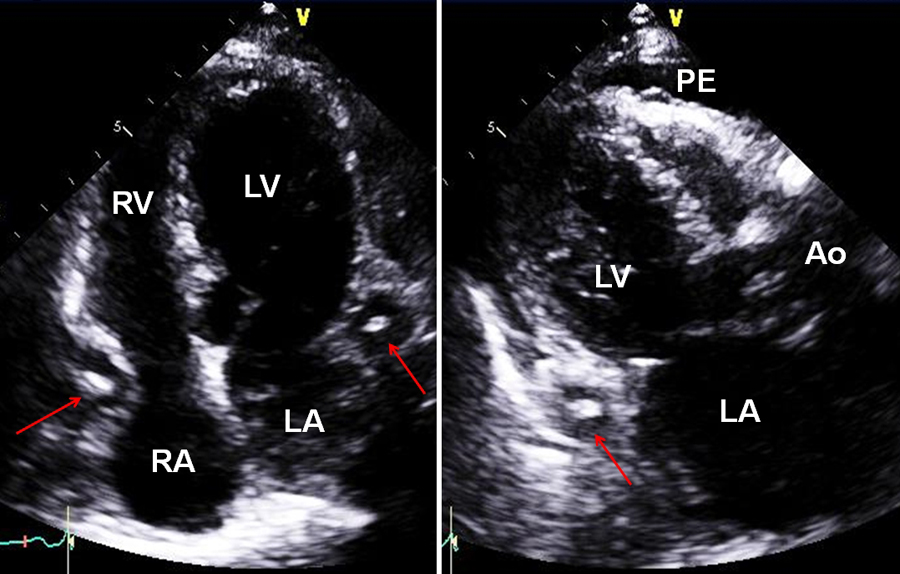
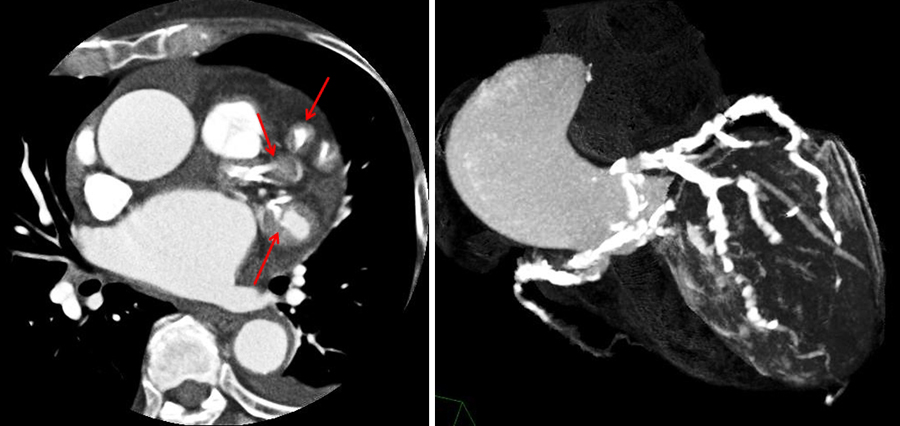
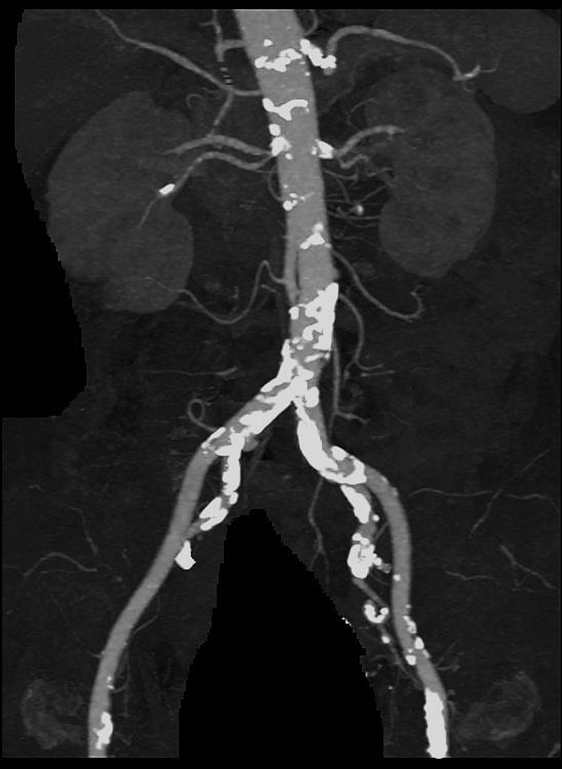
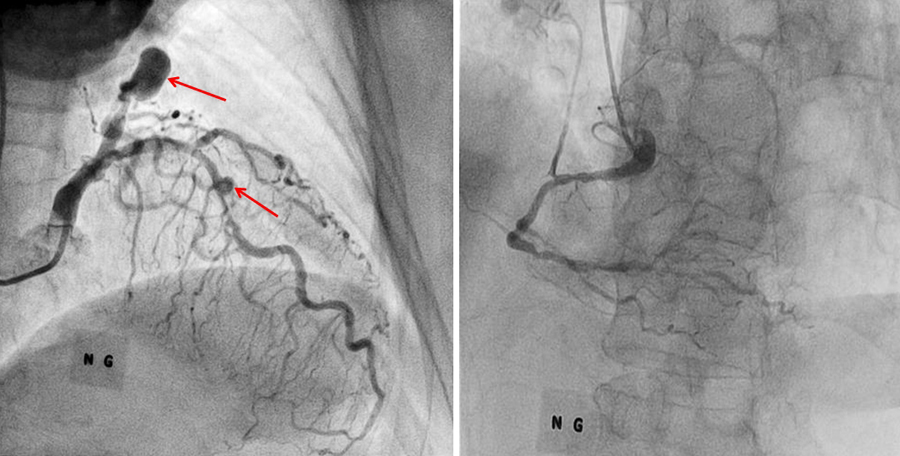
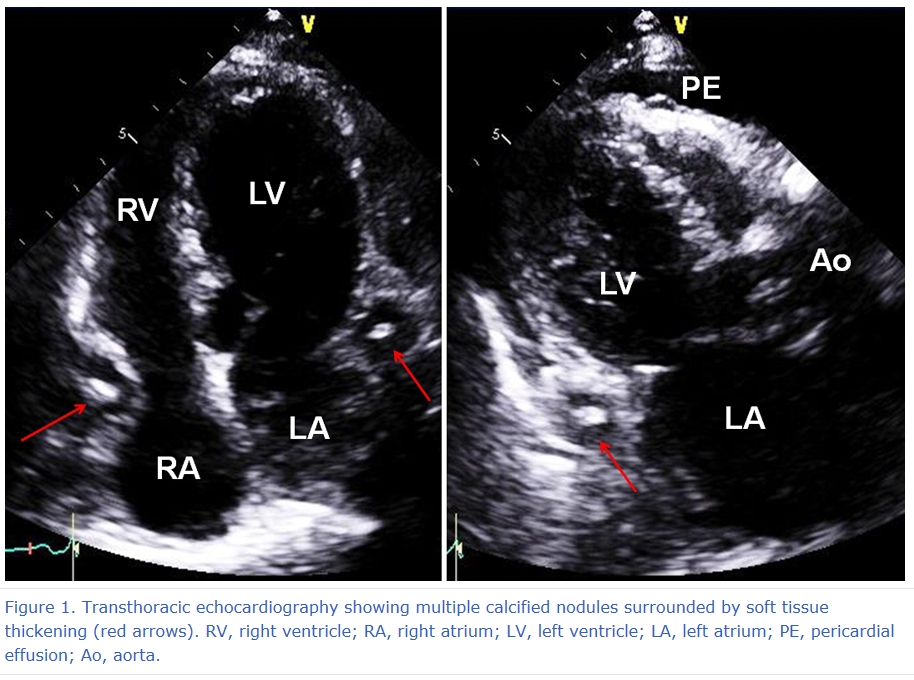
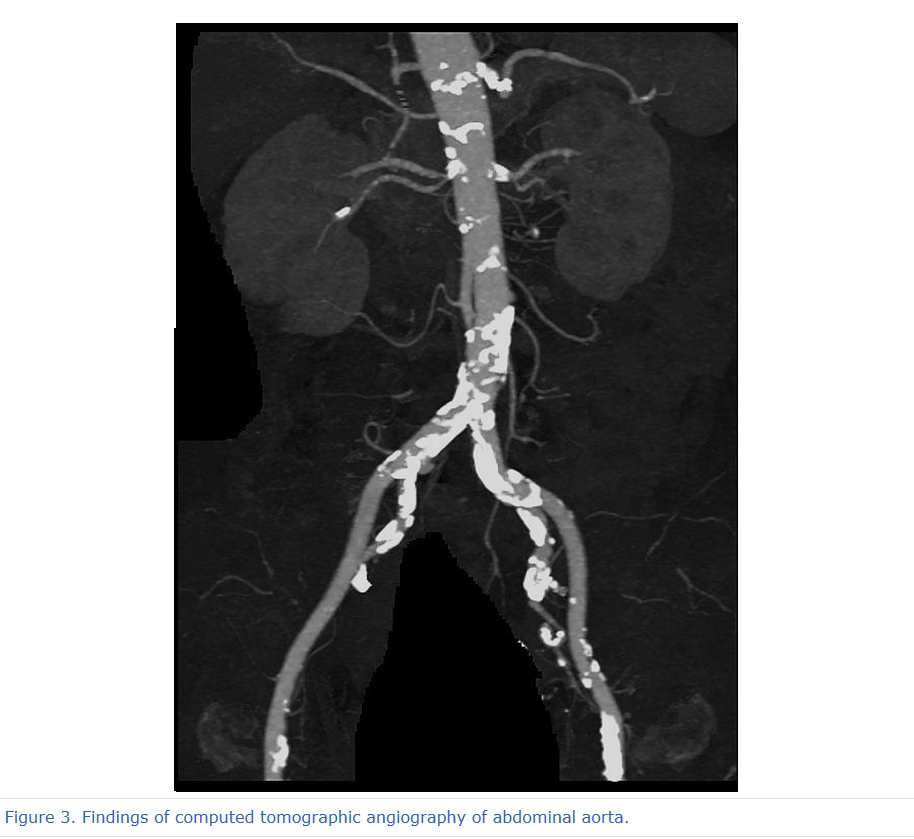
A 75-year old woman was referred to the Cardiology department to perform cardiac evaluation before total knee arthroplasty. She had no cardiac or chest symptoms. Her prior medical history was nonspecific except essential hypertension, which had been diagnosed several years ago. In her physical examination, there was grade III systolic murmur at right parasternal border. There were no other abnormal findings in her physical examination. Electrocardiogram and chest X-ray showed no abnormal findings. Transthoracic echocardiography showed multiple dense calcified nodules surrounded by soft tissue density with low echogenicity (Figure 1). There was moderate degree aortic stenosis and small amount of pericardial effusion. Size and function of left ventricle were normal. Coronary CT angiography was performed and it revealed that extensive calcification of all three coronary arteries (Figure 2). There were also diffuse and multiple low attenuated soft tissue thickening around coronary arteries (Figure 2). Although we did not detect aneurysmal dilatation of the aorta, total aorta CT showed extensive calcification of entire aorta (Figure 3). No other apparent abnormality was found in her abdomen in CT imaging. Invasive coronary angiography demonstrated multiple significant stenosis and aneurysms of left anterior descending and left circumflex coronary arteries. The proximal portion of right coronary artery was ectatic (Figure 4). The concentration of IgG4 was markedly elevated in her serum as 503 mg/dL (reference range, 6.1~121.4 mg/dL). Although tissue confirm was not performed, IgG4-related periarteritis of coronary artery could be diagnosed from the imaging and serologic findings. Treatment of oral corticosteroid (prednisolone 30 mg/day) and azathioprine (50 mg/day) were initiated.
This case suggested that IgG4-related periarteritis could occur in the coronary artery. Coronary artery involvement of IgG4-related disease can be fatal, if untreated. However, fortunately, most forms of IgG4-related disease respond well to corticosteroids, even in advanced stage. Therefore, early diagnosis and treatment is very important. When encountered unusual findings of coronary artery morphology such as extensive calcification with surrounding soft tissue swelling and aneurysmal formation, a careful consideration should be given to the possible diagnosis of IgG4-related disease involving coronary artery.
|
|||||||||||||
| 첨부파일1 | |||||||||||||
| 첨부파일2 | |||||||||||||

- Tel 02-3275-5258
- Fax 02-3275-5259
- E-mail herz1@circulation.or.kr
- Copyright© The Korean Society of Cardiology


- 심장학 최신지견 따라잡기
- 진료지침

{kind=link}
{kind=link}
{kind=link}
{kind=link}